RIte @ Home Program Standards, page updated Aug 20.2021
APPENDIX I: RIte @ Home Reimbursement Codes and
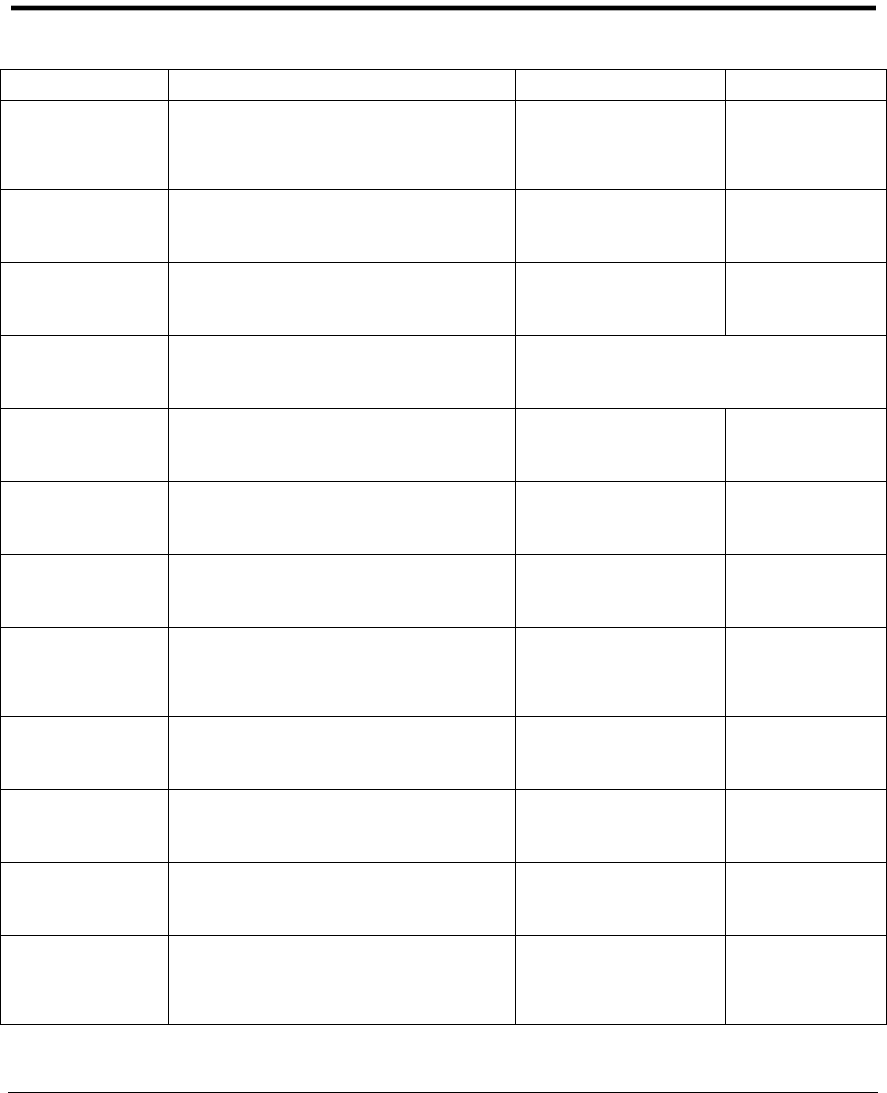
Rates for Fee-for-Service Medicaid
Executive Office of Health and Human Services
Rates Effective March 1, 2018
Code
Description
High LOC
Highest LOC
T2025
Case Management Admin, per
diem
high LOC
$ 26.03
N/A
T2025L1
Case Management/Admin, per
diem, highest LOC
N/A
$ 26.99
T1028
Development of Initial Service
and Safety Plan
$300.00
$300.00
T1005
Respite, per 15-minute units
Pay as Billed, up to $3,000
maximum per recipient per year
S5136U1
Stipend, per diem, high LOC, no
adult day
$41.80
N/A
S5136U1UN
Second participant stipend, per
diem, high LOC, no adult day
$31.35
N/A
S5136
Stipend, per diem, high LOC,
client attended adult day
$35.53
N/A
S5136UN
Second participant stipend, per
diem, high LOC, client attended
adult day
$26.65
N/A
S5136TGU1
Stipend, per diem, highest LOC,
no adult day
N/A
$52.92
S5136TGU1UN
Second participant stipend, per
diem, highest LOC, no adult day
N/A
$39.70
S5136TG
Stipend, per diem, highest LOC,
attended adult day
N/A
$44.98
S5136TGUN
Second participant stipend, per
diem, highest LOC, attended
adult day
N/A
$33.74

RIte @ Home Program Standards, page updated Aug 20.2021
APPENDIX II: RIte @ Home Program Client Rights and
Responsibilities
Executive Office of Health and Human Services

RIte @ Home Program Standards, page updated Aug 20.2021
RIte@Home
Client Bill of Rights
Executive Office of Health and Human Services
Each Client has the Right to:
1. Be treated as an adult with respect and dignity;
2. Be fully informed of all client rights and responsibilities by the shared living
agency;
3. Be encouraged and assisted to exercise constitutional and legal rights
including the right to vote;
4. Be informed of his/her medical condition and the right to refuse treatment;
5. Receive appropriate and professional care in accordance with physician’s
orders, and receive prompt medical care as needed;
6. Be free from mental and physical abuse;
7. Complete privacy when receiving treatment or personal care;
8. Associate and communicate privately with any person of choice and send
and receive personal mail unopened;
9. Have access to and participate in activities of social, religious, and
community groups;
10. Have medical and personal information kept confidential;
11. Keep and use a reasonable amount of clothing and belongings, and have a
reasonable amount of private, secure storage space,
12. Manage own financial affairs unless unable to do so;
13. Be free of financial exploitation. The provider must not charge or ask for
applications or non-refundable deposits or solicit, accept, or receive money
or property from a client, other than the amount agreed to for services;
14. Receive a written agreement regarding services to be provided and any fees
or costs that care recipients may be responsible for;
15. A safe, secure, and supportive environment;
16. Be free of discrimination regarding race, color, national origin, sex, sexual
orientation, religion, or gender orientation;
17. Make suggestions or complaints without fear of retaliation;
18. Receive visitors at any time while being respectful of others in the household

RIte @ Home Program Standards, page updated Aug 20.2021
19. Have access to a telephone within the home setting and privacy while using
the phone. Arrangements for use of the phone for calls that may have a
charge are to be set by the participant and Shared Living provider.
20. Have services and supports explained to you in a manner which you can
understand;
21. Decide what kinds of services and supports you need and want;
22. Have your records and involvement with the Shared Living provider kept
confidential;
23. See all files related to you, including your case record, medical, and
professional reports, and obtain a copy of your record if desired;
24. Make decisions that will affect your life, including the right to design your
own individualized plan, to choose the people who assist in the development
of the plan and the right to provide informed consent to the implementation
of the plan, or have an advocate provide informed consent on your behalf;
25. Religious freedom and the right to religious practice of their choice;
26. Be protected from abuse, neglect, or mistreatment, financial exploitation,
unnecessary restraint or coercion and all other violations of human rights.
I have reviewed and understand the client bill of rights:
________________________________________ ______________________
Shared Living Participant Date
________________________________________ ______________________
Legal Guardian /Power of Attorney Date
________________________________________ _______________________
Caregiver Date
_______________________________________ _______________________
Shared Living Agency Representative Date

RIte @ Home Program Standards, page updated Aug 20.2021
APPENDIX III: Participant Agreement Form
Executive Office of Health and Human Services

RIte @ Home Program Standards, page updated Aug 20.2021
RIte@Home Program Participant Agreement
Executive Office of Health and Human Services
Participant Agreement Form
The purpose of this agreement is to describe the expectations of the “participant”, and
clarify the responsibilities of the RIte@Home provider, and the RI Executive Office of
Health and Human Services (EOHHS).
In considered of the services provided through EOHHS I understand and agree to
following:
1. I have been informed of the responsibilities and expectations required by
_____________________ RIte@Home Agency and acknowledge that my
participation in the RIte@Home Program is voluntary.
2. I understand that under the rules of the RI Medicaid program and EOHHS, I have
been determined eligible for Long Term Care and the RIte@Home program.
3. I understand that my level of care and my service and safety plan will be
reviewed on an annual basis.
4. I understand that at any time, if my medical care and /or personal care needs are
cannot be safely provided for within the guidelines of the RIte@Home program,
alternative programs or placements will be presented to me. This change maybe
the result of hospitalizations or a gradual worsening of a chronic condition and
requires care not available to a participant of the RIte@Home program.
5. I understand that I may terminate my RIte @Home services with this provider
and agree that I will provide 30 days’ notice for the termination of services. I also
understand that the RIte@Home agency may involuntarily disenroll me from the
program for reasons listed in the program standards.
By signing this document, I acknowledge that if my needs change and I require a
higher level of care than can be provided by the RIte@Home program I may not
continue participation in the RIte@Home program and these services will no longer be
authorized by EOHHS.

RIte @ Home Program Standards, page updated Aug 20.2021
I have had sufficient opportunity to review this entire document by reading or having
it explained fully in language I understand and I agree to be bound by its terms.
Signature of Participant: ________________________________________________
Print Name:__________________________________________________________
Address: _____________________________________________________________
Date:_________________________
Signature of Agency Representative:__________________________________________
Print Name: _____________________________________________________________
Date:__________________________

RIte @ Home Program Standards, page updated Aug 20.2021
APPENDIX IV: RIte @ Home Program Management of
Recipient Needs Report
Executive Office of Health and Human Services

RIte @ Home Program Standards, page updated Aug 20.2021
Date:
RIte@Home Program Management of Recipient Needs Report
Executive Office of Health and Human Services
RIte @ Home Provider Agency
Report Submission Date:
Table 1: Rite @ Home Caseload Activity Report
Month
Active Caseload
Suspended
Discharged
Unique Individuals
Name
CI Filed
January
February
March
April
May
June
July
August
September
October
November
December
Table 2: RIte @ Home Suspended Cases by Reason
Month
In Hospital
Temporary
NH/ Rehab
Other
Total
Name
CI Filed
January
February
March
April
May
June
July
August
September
October
November
December

RIte @ Home Program Standards, page updated Aug 20.2021
Table 3: RIte @ Home Discharge Cases by Reason
Month
Deceased
Permanent
Placement
in a NH
Voluntary
Withdrawal
No Longer MA
Eligible
Total
Name
CI Filed
January
February
March
April
May
June
July
August
September
October
November
December
Table 4: RIte @ Complaint Report by Reported by:
Month
Caregiver
Recipient
Family
Friend/Other
Complaint Reason/Detail
Resolved
Date
January
February
March
April
May
June
July
August
September
October
November
December
Notes:
Active Caseload: Approved case receiving services on the last day of the reported month.
Suspended: Approved case temporarily suspended on the last day of the month.
Discharged: Cases discharged from Shared Living in the reported month.
Unique Individuals: Active Caseload + Suspended Cases + Discharged Cases
RIte @ Home Provider Agency:
Report Submission Date:

RIte @ Home Program Standards, page updated Aug 20.2021
APPENDIX V: Caregiver Statement of Responsibility and
Understanding
Executive Office of Health and Human Services

RIte @ Home Program Standards, page updated Aug 20.2021
Caregiver Statement of Responsibility - Agreement and Understanding
I ____________________________, have been informed of the responsibilities and
expectations required by ________________________________(RIte @ Home Provider
Agency) for the RIte @ Home Program under the program standards set forth by the Executive
Office of Health and Human Services As a RIte @ Home caregiver, I agree to provide care and
supervision for _____________________________, at the location of
______________________, ___________________, RI.
As a RIte @ Home caregiver, I agree to provide twenty-four hour care and supervision to the
above noted care recipient unless relieved by an approved “secondary” or “respite” caregiver.
I also understand that all care recipient, caregiver or respite caregiver status changes, including,
but not limited to health status, living arrangement, financial situation, employment status,
provision of home care or hospice services, must be immediately reported to:
________________________________(RIte @ Home Provider Agency).
All changes in household residents, even those considered temporary (minors and adults), must
be reported to ________________________________(RIte @ Home Provider Agency) within
24 hours.
I understand that failure to notify _______________________________(RIte @ Home Provider
Agency) of status changes for the care recipient and caregivers may result in termination from
the EOHHS RIte @ Home Program. I also understand that under the state of Rhode Island
General Laws, Section 40-6-15, a maximum fine of $1,000, or imprisonment of up to five (5)
years, or both, may be imposed for a person who obtains or attempts to obtain, or aids or abets
any person to obtain, public assistance to which s/he is not entitled, or who willfully fails to
report income, resources or personal circumstances or increases therein which exceed the
amount previously
reported.
______________________ _____________________ ____________________
Primary Caregiver Printed Name Primary Caregiver Signature Date
In the presence of:
______________________ _____________________ ____________________
RIte @ Home Provide Agency Rep Signature RIte @ Home Rep Date

RIte @ Home Program Standards, page updated Aug 20.2021
APPENDIX VI: RIte @ Home Review Sheet
Rhode Island Executive Office of Health and Human Services

RIte @ Home Program Standards, page updated Aug 20.2021
OHHS SHARED LIVING SERVICE AND SAFETY PLAN REVIEW SHEET
SSP Received Date:
Participant Name:
MID:
DOB:
Care Giver Homes Fax: 489-7579
Seven Hills RI Fax: 765-2431
DHS LTC Supervisor:
Phone:
Fax:
Present
Missing
Dated cover sheet and narrative summary: Includes S/L agency documentation that either:
Client/Caregiver/host home are unconditionally recommended for S/L without reservation.
Client/Caregiver/host home are recommended for S/L with conditions (List Conditions).
Completed S/L Service and Safety Plan: Includes signed and dated contract with:
S/L agency RN signature S/L Client signature S/L Caregiver Signature
Plan of Care: (prioritized, unduplicated domains/goals) with detailed S/L agency RN and SW
visit
schedule and detailed caregiver and respite provider responsibilities.
Medication List: (current and complete) including nutritional supplements and OTC products,
herbal
supplements, with side effects and participant’s DX/reason for medication.
Assessments and medical documentation:
Nursing Assessment Social Service Assessment PM-1 (required upon initial)
PM-1 or last PCP office visit documentation for reauthorization of SSP.
Home Owner Insurance: Documentation of home owner insurance
Transportation Arrangements: Includes arrangements between parties, safe driving
record
documentation and proof of current auto liability insurance.
Safe Evacuation: includes documentation that participant can be evacuated safely per service
and
safety plan.
BCI Documentation:
caregiver
respite provider all individuals over 18 living in S/L host
home
Physician’s statement of adequate health: Includes documentation of physical
limitations
and TB screen (every 2 years)
caregiver
respite provider
Competency Check List:
caregiver
respite provider
First Aid and CPR Certification (every 2 years): Proof of current certifications. caregiver
respite provider copy of comfort one certificate (waive requirements)
DEA Adult Protective Services Inquiry: (60 plus)
S/L Bill of Rights and Responsibilities: signed and submitted
S/L Status Form Turnaround (OHHS S/L -2) complete by LTC
Gratuitous Nursing Statement Signed by:
caregiver
S/L participant
Plan is approved; effective start date:
Next S/L effective start date:
Plan approved, current Core Services S/L effective start date:
Plan is Not approved; additional information of response required within 5 calendar days from:
Plan is Not approved (see comments below)
Reviewer Name/Title:
Phone:
Fax:
Signature:
Fax date:
Comments:

RIte @ Home Program Standards, page updated Aug 20.2021

RIte @ Home Program Standards, page updated Aug 20.2021
APPENDIX VII: RIte @ Home Fact Sheet
Executive Office of Health and Human Services

RIte @ Home Program Standards, page updated Aug 20.2021
RIte @ Home…
A Choice for Care at Home
fact sheet
Program Description
RIte @ Home… A Choice for Care at Home is a new RIte @ Home option available for adults who
cannot live alone and require a considerable amount of help with the activities of daily living,
such as eating, dressing, personal hygiene, etc. This program provides an alternative to
institutional care for those that meet clinical, financial and other program criteria. The RIte @
Home Program is a person-centered service designed to maximize the control and choice a
person has over the services that are provided. It is provided through the Medicaid Program at
the Executive Office of Health and Human Services (EOHHS).
Eligibility
This service is available for Rhode Island seniors and adults with disabilities who are eligible for
Medicaid Long Term Care (LTC) and are unable to live independently. To be eligible for
Medicaid LTC, a person has to be determined financially eligible and must also meet certain
clinical Level of Care criteria (highest or high). Persons interested in receiving RIte @ Home
services must also meet all appropriateness criteria listed below.
How It Works
RIte @ Home provides a home-like setting for individuals who cannot live alone but who want
to continue to live in the community as long as possible. There are two components to
understanding the program: (1) the provider agency and (2) the caregiver and the home setting.
Provider Agency

RIte @ Home Program Standards, page updated Aug 20.2021
The RIte @ Home Agency helps the person who needs care to find an appropriate home
setting/caregiver. This may be someone the person already knows, like a relative, neighbor or
friend. The Agency will “match” a client with a caregiver and will make sure the caregiver
receives all needed training and support.
The Agency will (in conjunction with EOHHS)
• Oversee and monitor services;
• Ensure the safety of the home setting;
• Provide training for the caregiver;
• Provide nursing support as needed, and
• Develop an individualized RIte @ Home Service and Safety Plan.
The Caregiver/Home Setting
Typically, the caregiver lives in his/her home and agrees to have the person needing care live
with him/her. In some situations, the caregiver may agree to move into the care recipient’s
home. The Caregiver is responsible for:
• Personal care, including assistance with Activities of Daily Living (ADLs)
• Homemaker services
• Chore services
• Meals
• Transportation
• Being on call 24/7
• Providing socialization and a home-like environment
Benefits for the Caregiver include:
A stipend for providing 24/7 care
Respite or time off from full-time care
Medicaid pays the provider agency for its role and provides funding for caregiver stipends.
However, Medicaid does not pay for room and board. Room and board is typically paid from
the client’s SSI and/or Social Security check. Also, the client (recipient of care) may incur a “cost
share” for the services (not including room and board), depending on his/her income.
Appropriateness Criteria
Recipients must meet the following Appropriateness Criteria:
• A person is not a danger to themselves or others in the shared home.

RIte @ Home Program Standards, page updated Aug 20.2021
• A person must be able to take action for self-preservation (such as exiting the home
in case of fire) with the assistance of no more than one person.
• Both the caregiver and the recipient must be informed of and willing to assume a
certain amount of risk regarding safety inherent in this type of living arrangement.
• A recipient must be free from communicable disease or infectious conditions.
Other Considerations
Spouses or legally liable persons cannot serve as the paid caregiver.
Adult Day Care - The recipient of RIte @ Home Services is eligible to attend Adult Day Care. If
that is the case, the caregiver’s stipend will be reduced for days when a person attends Adult
Day Care. This gives the caregiver an opportunity for employment or pursuing other interests.
Issues to be considered when matching a person to a caregiver:
• Geographic location
• Pets
• Children in the home
• Lifestyle preferences, schedules, etc.
Tax Considerations- The Caregiver’s stipend is tax-free to the Caregiver when the care recipient
lives in the Caregiver’s home.
Provider Agencies
Two agencies have been approved to provide RIte @ Home services to eligible elders and adults with
disabilities:
Caregiver Homes of Rhode Island
Contact: Nelia Botelho, MSW; District Manager at (401) 473-2794 or
nbotelho@caregiverhomes.com
Colleen DeGroot, MSW; Clinical Practice Manager at (401) 473-2159 or
cdegroot@caregiverhomes.com
235 Promenade St., Suite 417, Providence, RI 02908
www.caregiverhomes.com
Seven Hills RI
Contact: Lisa Provencal, Program Coordinator, (401) 229-9760 or (401) 309-4093
lprovencal@sevenhills.org
68 Cumberland St., Suite 300, Woonsocket, RI 02895

RIte @ Home Program Standards, page updated Aug 20.2021
RIte @ Home…A Choice for Care at Home is one of the services available to clients who are eligible for
Medicaid Long Term Care. For more information on other services, please go to the DHS website at
under Elders>Long Term Care or Adults with Disabilities Long Term Care Program
