
The United Republic of Tanzania
Ministry of Health and Social Welfare
Reproductive and Child Health Section. March 2010
2010 - 2015
National Family Planning
Costed Implementation Program
Reproductive & Child Health Section. March 2010
This publication is made possible by the generous support of the American people through the
United States Agency for International Development (USAID).

United Republic of Tanzania | National Family Planning Costed Implentantation Program
United Republic of Tanzania | National Family Planning Costed Implentantation Program
UNITED REPUBLIC OF TANZANIA
The National Family Planning
Costed Implementation Program
2010 - 2015
Ministry of Health and Social Welfare

United Republic of Tanzania | National Family Planning Costed Implentantation Program

United Republic of Tanzania | National Family Planning Costed Implentantation Program
Table of Contents
Abbreviations ...................................................................................................................................... i
Foreword ............................................................................................................................................ii
Acknowledgments ..............................................................................................................................iv
Executive Summary ............................................................................................................................ 1
Introduction ....................................................................................................................................... 4
National Family Planning Costed Implementation Program .................................................................. 13
Purpose of the NFPCIP ............................................................................................................ 13
Vision, Mission, Goals and Objectives of the NFPCIP .................................................................. 14
Analysis of Demographic Determinants of Resource Requirements ............................................. 16
Strategic Actions to Achieve Objectives ..................................................................................... 23
Institutional Arrangements for Implementation ................................................................................... 32
Resource Mobilization Framework ............................................................................................ 33
Monitoring and Evaluation of Plan Implementation ..................................................................... 34
Appendices .................................................................................................................................... 35
Appendix A: 2009–2010 Family Planning Partners and Implementers ..................................36
Appendix B: Summary Report of Key Informant Interviews and Advance Consultations ...........37
Appendix C: Summarized Process for Development of NFPCIP ..............................................42
Appendix D: Definition of Terms Used in the NFPCIP and Analytical Framework ......................45
Appendix E: Annual Resource Requirements by Strategic Action Area ...................................47
Appendix F: Bibliography ...................................................................................................66

United Republic of Tanzania | National Family Planning Costed Implentantation Program

United Republic of Tanzania | National Family Planning Costed Implentantation Program
i
Abbreviations
ADB Asian Development Bank
ADDOs Accredited drug dispensing outlets
ANC Antenatal care
ACQUIRE ACcess, Quality, and Use In REproductive
health
BCC Behaviour change communication
CBD Community-based distribution
CBOs Community-based organizations
CBS Community-based services
CCHP Council Comprehensive Health Plans
CHMT Council Health Management Team
CIDA Canadian International Development Agency
CMT Country Management Team
CPR Contraceptive prevalence rate
CSOs Civil society organizations
CTU Contraceptive technology update
DfID Department for International Development
(United Kingdom)
DHS Demographic and Health Survey
DMPA Depot-medroxyprogesterone acetate
DRCHCo District Reproductive and Child Health
Coordinator
FBOs Faith-based organizations
FHI Family Health International
FP Family planning
GTZ Gesellschaft für Technische Zusammenarbeit
HMIS Health management information system
HPI Health Policy Initiative
HRHSP Human Resources for Health Strategic Plan
HSSPIII Health Sector Strategic Plan III
IEC Information, education and communication
IPPF International Planned Parenthood Federation
IUDs Intrauterine devices
KfW Kreditanstalt für Wiederaufbau
LAPMs Long-acting and permanent methods
LGAs Local government authorities
M&E Monitoring and evaluation
MCH Maternal and child health
MDGs Millennium Development Goals
MoFEA Ministry of Finance and Economic Affairs
MoHSW Ministry of Health and Social Welfare
MSD Medical Stores Department
MTEF Medium-Term Expenditures Framework
MWRA Married women of reproductive age
NBS National Bureau of Statistics
NFPCIP National Family Planning Costed
Implementation Program
NGOs Non-governmental organizations
NORAD Norwegian Agency for Development
Cooperation
PAC Post abortion care
PHSDP Primary Health Services Development
Programme
PNC Postnatal care
POPC President’s Office Planning Commission
PMO–RALG Prime Minister’s Office–Regional
Administration and Local Government
PROGRESS Program Research for Strenghthening
Services
PSI Population Services International
PSU Pharmaceutical Support Unit
RCHCo Reproductive and Child Health Coordinator
RCHS Reproductive and Child Health Section
RH Reproductive health
RMO Regional Medical Officer
RMT Regional Management Team
SAAs Strategic Action Areas
SAAWGs Strategic Action Area Working Groups
SDP Service delivery point
SIDA Swedish International Development
Cooperation Agency
SPAS Service Provision Assessment Survey
SRH Sexual and reproductive health
STIs Sexually transmitted infections
SWAps Sector-wide approaches
TACAIDS Tanzania Commission on AIDS
TFDA Tanzania Food and Drug Authority
T-MARC Tanzania Marketing and Communications
Company
THMIS Tanzania HIV/AIDS and Malaria Indicator
Survey
UMATI Chama Cha Malezi Bora Tanzania
UNFPA United Nations Population Fund
USAID United States Agency for International
Development
WHO World Health Organization
WRA Women of reproductive age
YFS Youth-friendly services

United Republic of Tanzania | National Family Planning Costed Implentantation Program
ii
Foreword
Family planning saves the lives of women, newborns, and adolescents as well as contributes to
the nation’s socioeconomic development. Family planning prevents maternal mortality, one of the
major concerns addressed by various global and national commitments and reflected in the targets
of the Millennium Development Goals, Tanzania Vision 2025, the National Strategy for Growth
and Reduction of Poverty, and the Primary Health Services Development Program, among others.
Family planning also reduces infant deaths from AIDS by preventing unintended pregnancies
and hence mother-to-child transmission of HIV. Family planning also helps governments achieve
national and international development goals because it can contribute to the achievement of all
of the United Nations’ Millennium Development Goals, including reducing poverty and hunger,
promoting gender equity and empowering women, reducing child mortality, improving maternal
health, combating HIV/AIDS, and ensuring environmental sustainability.
Over the last decade, however, other competing health priorities, such as tuberculosis, malaria, and
HIV/AIDS have reduced the resources and visibility enabling Tanzania’s family planning program
to keep pace with unmet needs for these services. As such, the momentum of family planning
programs has slowed considerably since 1999. Whilst modern method prevalence increased from
6.6 percent in 1992 to 13.3 percent in 1999, the annual increase in prevalence has dropped by 0.2
percentage points per year since then, with prevalence reaching only 26.4 percent in 2004–2005.
At the same time, Tanzania has faced rising demands for family planning services, increasing from
38.3 percent in 1991–1992 to 49.5 percent in 2004–2005.
The Ministry of Health and Social Welfare (MOHSW) developed this National Family Planning
Costed Implementation Program (NFPCIP) based on the goal of the One Plan to increase the
contraceptive prevalence rate to a target of 60 percent by the year 2015. The NFPCIP is also guided
by and links with the Health Sector Strategic Plan III (HSSPIII), the Human Resources for Health
Strategy Plan (HRHSP), and the Primary Health Service Development Programme (PHSDP). Funds
required to implement these NFPCIP activities will build on and augment the many investments
called for in the HSSPIII, PHSDP, and HRHSP strategies by ensuring that essential resources
for an effective family planning program are identified and that the activities are integrated and
implemented within and throughout the overall health system.
The main objective of the NFPCIP is to reposition and reinvigorate access to and use of family
planning services in Tanzania. The NFPCIP stipulates five strategic action areas for implementation
that are needed to reposition family planning: contraceptive security, capacity building, service
delivery, health systems management, and advocacy. Although all five components are needed for a
thriving and effective program, emphasis will be given to two areas to prioritize fulfilment of the
increasing demands for family planning services in the country. These two areas include ensuring
contraceptive security and strengthening integrated service delivery of family planning in all aspects
of the health sector, including HIV/AIDS, immunization services, postnatal care, and postabortion
care.
Implementation of this plan requires that strategies and actions be integrated into the medium-
term expenditure frameworks of government ministries and into the budgets of local government
authorities. It is also the expectation of the Government, particularly the MoHSW, that development
partners and all stakeholders will make optimal use of this NFPCIP to support the implementation
of a reinvigorated family planning program and reach our target rate of contraceptive prevalence of
60 percent by 2015.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
iii
Having developed the NFPCIP, the Government of Tanzania is strongly committed to its successful
implementation. All stakeholders have an obligation to participate to reposition and reinvigorate
access to and use of family planning services in Tanzania. We thank all stakeholders for working to
achieve the development of this plan. Together, we can improve the health of Tanzanian mothers,
babies, and children, and build a stronger and more prosperous nation.
Blandina S. J. Nyoni
Permanent Secretary
Ministry of Health and Social Welfare

United Republic of Tanzania | National Family Planning Costed Implentantation Program
iv
Acknowledgments
The Ministry of Health and Social Welfare (MoHSW) would like to express sincere gratitude to
the many individuals and development partners who worked with the Ministry to develop the
National Family Planning Costed Implementation Program. The completion of this document is a
result of extensive consultations and collaboration with various stakeholders, including other sector
ministries, development partners, professional associations, and interested organizations as well as
committed individuals and under the guidance of the National Family Planning Working Group.
The Ministry acknowledges the financial and technical support from the United States Agency for
International Development (USAID) for coordinating all activities that culminated in the NFPCIP
through the Program Research for Strengthening Services (PROGRESS) Project managed by Family
Health International (FHI) which provided secretariat support, technical guidance, and costing; and
through the Health Policy Initiative Project managed by the Futures Group which provided the
needed modeling and development of projections. Furthermore, the Ministry greatly appreciates
the technical support from EngenderHealth, John Snow Inc., Management Sciences for Health,
Marie Stopes Tanzania, Pathfinder International, Population Services International, T-MARC and
UNFPA for co-leading the development of strategic actions, together with Reproductive and Child
Health (RCHS) staff.
The Ministry recognizes and acknowledges the participation of many individuals from its development
partners (Donor Partners Group for Health and Gesellschaft für Technische Zusammenarbeit)
and from sectoral ministries (Ministry of Finance and Economic Affairs; Ministry of Community
Development, Gender and Children; President’s Office Planning Commission; Medical Stores
Department; and the National Bureau of Statistics). The MoHSW also appreciates the participation
and contributions of regional and district representatives for their inputs in the NFPCIP.
Finally, the Ministry would like to acknowledge the RCHS for leading the coordination of all
stakeholders engaged in the development process of this document.
Dr. Deo M. Mtasiwa
Chief Medical Officer
Ministry of Health and Social Welfare
United Republic of Tanzania | National Family Planning Costed Implentantation Program
1
Executive Summary
Meeting the ‘One Plan’ Goal for Family Planning
A continuing high rate of population growth is presenting major challenges to social and economic
development in Tanzania. According to the National Bureau of Statistics (NBS), at the current
annual rate of growth of 2.9 percent, Tanzania’s population is projected to reach 65 million by 2025,
putting increased strain on already overstretched health and education services, infrastructure, food
supply, and the environment. Early initiation of childbearing and a high rate of fertility are the
principal factors contributing to this rapid population growth, and they also have detrimental effects
on the health of women and children. Tanzania has among the highest rates of maternal, newborn,
and child deaths in the world. Gender issues play important roles in both affecting access to health
and economic resources for women and limiting the roles women can play in the country’s social
and economic development. Early childbearing usually curtails educational attainment for girls and
constrains women’s participation in economic productivity.
Family planning (FP) has for several decades been well documented as a key strategy to promote
social and economic development, and to improve the health of women and their children. The
National Road Map Strategic Plan to Accelerate Reduction of Maternal, Newborn and Child Deaths in
Tanzania, 2008–2015 (One Plan) has set a goal to increase the contraceptive prevalence rate (CPR)
from 20 percent to 60 percent by 2015, by making quality FP services more accessible to and
equitable for all of Tanzania’s people. Increased use of FP has a great potential to contribute to the
One Plan target of reducing maternal mortality from 578 to 193 per 100,000 live births by 2015.
However, the Tanzania’s FP program has lost momentum over the past decade because of a number
of factors. As a result, the national CPR for modern methods among married women of reproductive
age at the time of the last Demographic and Health Survey (DHS) in 2004–2005 had reached only
20 percent, and the annual rate of growth in CPR had slowed from a high of 1.5 percentage points
to 0.6 percentage points. With the current level of investment in FP and the current rate of growth,
the One Plan target will not be reached until 2030, with considerable negative consequences for
the health and well-being of Tanzania’s people and increased challenges to the country’s economic
development. It was noted in a recent study on National Health Accounts that expenditures for
FP had decreased drastically, from 54 percent of reproductive health (RH) spending in 2003 to 8
percent in 2006. Deliberate efforts must be taken to rectify the situation. A renewed commitment
to FP, a reinvigorated program, and significant investment of resources are thus required to achieve
the One Plan target.
In recognition of the need to reinvigorate the national FP program, the Ministry of Health and
Social Welfare (MOHSW) embarked on development of a costed implementation program for
a ‘repositioned’ national FP program. The National Family Planning Costed Implementation
Program (NFPCIP) is guided by the vision and mission of the Reproductive and Child Health Policy
Guidelines 2003 and the goals of the one plan, setting targets for increased use of all FP methods by
all women of reproductive age. The NFPCIP takes into consideration and builds on the substantial
investments called for in other strategic plans and documents, namely the Health Sector Strategic
Plan III (HSSPIII) July 2009–June 2015, the Primary Health Services Development Programme
(PHSDP) 2007–2017, and the Human Resources for Health Strategic Plan (HRHSP) 2008–2013.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
2
Through a collaborative, participatory, and consultative process involving a wide range of stakeholders,
five strategic action areas (SAAs) have been defined, based on the issues and challenges that must
be addressed to reposition FP successfully. These are ensuring contraceptive commodities and
logistics (adequate and timely supplies of contraceptive methods appropriate to meet individual
needs); renewed efforts in capacity building to ensure that providers in the health sector have the
skills required to provide and support integrated FP services; strengthened service delivery systems
to increase access to quality, affordable, and sustainable services; a renewed focus on advocacy to
increase visibility of and support for FP among development partners, program managers, service
providers, and the public; and strengthening management systems, monitoring and evaluation
(M&E) to ensure effective program implementation.
Estimating the Level of Financial Support for Repositioning Family
Planning
Table 1 provides a summary of funding in Tanzanian shillings and U.S. dollars needed each year
through 2015, by Strategic Action Area (SAA), to reach a national average CPR target of 60 percent
for all methods for all women of reproductive age by 2015. Guided by an analytical framework
that projects needs based on the current population structure and growth rates, and considers the
diverse situations in mainland Tanzania’s 21 regions, these estimates were derived through an
iterative process to define and prioritize activities that will be required to achieve the objectives in
each of the five SAAs. Through this process, a total of 28 strategic actions were defined across all five
areas. These were further broken down into specific activities, with timelines and inputs required
for implementation. Unit costs of the inputs were then used to estimate the cost for each activity
each year.
The activities and the costs of the inputs needed for each SAA serve as a platform for mobilizing
resources as well as for tracking implementation and measuring the impact of the NFPCIP. Careful
review of the HSSPIII, PHSDP, and HRHSP have been undertaken to ensure no duplication of the
investments and that the NFPCIP is integral of these strategic health programs. Although
investments in these strategic health programs will benefit the entire health sector, including FP,
the resource needs identified in the five SAAs of the NFPCIP are the additional investments that
will be required specifically to strengthen FP through a coordinated approach to achieve the One
Plan target.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
3
Table 1. Annual Funding Requirements, 2010–2015, by Strategic Action Area to Reposition Family Planning, with 60 percent CPR Target Achieved by 2015 (in Tshs/USD)
STRATEGIC ACTION AREA
FISCAL YEAR
TOTAL COST
ESTIMATE
FY 2010–2011 FY 2011–2012 FY 2012–2013 FY 2013–2014 FY 2014–2015 FY 2015–2016
I. Contraceptive security & logistics 16,282,691,047 17,592,358,355 18,700,234,439 20,617,616,767 22,733,318,127 25,403,005,311 121,329,224,046
II. Capacity building 1,211,037,000 1,619,613,533 913,909,250 730,794,500 604,212,000 604,112,000 5,683,678,283
III. Service delivery 465,895,283 917,230,750 570,577,000 96,353,750 99,935,000 64,000,000 2,213,991,783
IV. Advocacy 1,129,514,330 583,857,580 743,772,250 133,831,250 133,831,250 118,047,750 2,842,854,410
V. Management systems/M&E 549,527,800 202,613,800 134,500,300 77,746,300 72,346,300 84,496,300 1,121,230,800
Total (in Tshs) 19,638,665,461 20,915,674,018 21,062,993,239 21,656,342,567 23,643,642,677 26,273,661,361 133,190,979,323
Total (in USD$) 14,547,160 15,493,092 15,602,217 16,041,735 17,513,809 19,461,971 98,659,985
Exchange rate: 1 USD = 1,350 Tshs.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
4
Introduction
Background
The health benefits of Family Planning (FP) for women and their children have been well documented
for several decades, as has its essential contributions to social and economic development. Limited
FP services have been available in a few urban areas of Tanzania since the establishment of the
family planning association of Tanzania (UMATI) in 1959. Beginning in 1974, the Government of
Tanzania allowed UMATI to expand FP services to public-sector maternal and child health (MCH)
clinics throughout the country, but expansion was limited because of resource constraints, and levels
of contraceptive use remained low.
Expansion of the program and growth in the contraceptive prevalence rate (CPR) were accelerated
after a speech by the late first President Julius Kambarage Nyerere in 1989 that recognized
the importance of FP to Tanzania’s development. In 1989, the Tanzanian government assumed
responsibility for integrating FP into government MCH services from UMATI. During the next
few years—the ‘golden age’ of FP in Tanzania—the prevalence of modern FP method use more than
doubled, increasing from 6.6 percent in 1992 to 13.3 percent in 1996, growing at an average of 1.5
percentage points per year. Beginning in 2000, however, the increase in prevalence dropped to 0.6
percentage points per year, with contraceptive prevalence for all methods among married women of
reproductive age reaching only 26.4 percent by the time of the last Demographic and Health Survey
(DHS) in 2004–2005.
A number of factors contributed to the loss of momentum, including decentralization and integration
of health programs and the shift in donor funding mechanisms and priorities. As FP priority,
visibility, and financial support declined, the fundamental elements needed to sustain a thriving
FP program were also weakened at central, regional, and district levels. These elements include a
consistent and adequate supply of contraceptive commodities to meet increasing demand, capacity
building to increase the number of skilled FP providers and ensure updated provider skills, well-
equipped and flexible service delivery systems, education and motivation to generate demand for
services, advocacy to sustain support for FP from various funding sources, and effective management
systems and leadership to guide program implementation.
Repositioning FP as a priority in the national agenda is a key strategy to improve maternal, newborn,
and child health; to prevent mother-to-child HIV transmission; and to promote social and economic
development. Renewed advocacy for FP and adequate funding for program implementation to meet
these goals are therefore urgently needed.
Health and demographic indicators are the widely accepted measures used to assess a country’s
health situation. Key indicators for Tanzania are shown in Table 2. Tanzania has a young population,
with early childbearing and high rates of fertility continuing throughout reproductive life. These
factors account for the projected near-doubling of the population by 2025, placing increasing stresses
on health and education systems, availability of food and clean water, natural resources and the
environment, and economic growth and development. All of the girls who will enter childbearing
age over the next decade have already been born, and with almost half of the country’s population
United Republic of Tanzania | National Family Planning Costed Implentantation Program
5
under age 15, Tanzania’s population growth will only accelerate. Early initiation of childbearing and
numerous, closely-spaced pregnancies throughout a woman’s reproductive life contribute not only
to rapid population growth but also to adverse social consequences such as gender inequity. Girls
who experience their first pregnancy during adolescence often terminate their education, limiting
their future participation in positive social and productive economic activity. In addition, early and
frequent childbearing has serious health consequences for girls and women, contributing to higher
rates of complications such as eclampsia, obstructed labour, haemorrhage, anaemia, premature
delivery, and death.
Table 2. Tanzania Demographic and Health Indicators
INDICATOR
Population in millions, Tanzania mainland (2002 census) 34.4
Projected population in millions, 2004, Tanzania mainland (2004–2005 DHS) 36.0
Projected population, 2025, in millions (NBS) 65.3
Annual population growth rate (2002 census) 2.9
Percent of population under age 15 (2002 census) 47.0
Percent of women pregnant or with live birth by age 19 (2004–2005 DHS) 52.0
Total fertility rate (2004–2005 DHS) 5.7
CPR, modern methods (2004–2005 DHS) 20.0
Unmet need for FP (2004–2005 DHS) 21.8
Maternal mortality per 100,000 live births (2004–2005 DHS) 578
Infant mortality per 1,000 live births (2007 THMIS) 58
DHS = Demographic and Health Survey; NBS = National Bureau of Statistics; THMIS = Tanzania HIV/AIDS and
Malaria Indicator Survey.
Maternal mortality rates in Tanzania are among the highest in the world. Abortion is illegal in
Tanzania, and abortion complications are estimated to contribute to about 16 percent of maternal
deaths. Family planning services can significantly reduce unintended pregnancies and maternal
mortality from unsafe abortions. Maternal mortality rates in Tanzania could be reduced by as much
as 35 percent if the One Plan FP goal is achieved.
High rates of infant and child deaths are another consequence of early and frequent childbearing
and of childbearing late in life (after age 35). Despite significant progress in reducing the infant
mortality rate, this rate remains high in Tanzania. Significant reductions in infant mortality can also
be realized by a reinvigorated FP program, saving the lives of half a million children over a 10-year
period.
Access to safe, effective, acceptable, and affordable FP methods and services is a key, highly cost-
effective intervention to save lives and reduce the adverse social and economic consequences of rapid
population growth. As shown in Table 2, at the time of the 2004–2005 DHS, more Tanzanian
women expressed an unmet need for FP than were actually using an FP method. An estimated
2.9 million unintended pregnancies could be averted over the next decade if the unmet need for
contraception were met. Although achieving the One Plan target will require increased demand for
FP, meeting the currently high level of unmet need alone would make a substantial contribution
toward achieving the goal.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
6
Increased availability and use of FP is a key strategy for preventing HIV/AIDS. Consistent and
correct use of condoms is an important means of preventing transmission of HIV and other sexually
transmitted infections (STIs). Family planning is also a highly cost-effective means of preventing
mother-to-child transmission of HIV (PMTCT). Among infected women who do not wish to become
pregnant, providing effective contraception to prevent an unintended pregnancy costs a fraction of
providing antiretroviral drugs for PMTCT or of caring for AIDS orphans.
Investments in FP will contribute substantially to achievement of six of the eight Millennium
Development Goals (MDGs): reducing poverty and hunger, promoting gender equity and empowering
women, reducing child mortality, improving maternal health, combating HIV/AIDS, and ensuring
environmental sustainability. Family planning is a priority in the national development agenda, and
its visibility must be enhanced so that increased access to and use of FP methods and services can
make important contributions to achieving the country’s overall health and development goals.
An estimated 80 percent of FP services are provided by decentralized public-sector health facilities
through 133 local government authorities (LGAs). These include regional and district hospitals,
health centres, dispensaries, and community health services. In addition to the public-sector facilities,
a number of hospitals, health centres, and dispensaries managed by faith-based organizations
(FBOs) and standalone FP/RH clinics managed by nongovernmental organizations (NGOs) also
provide FP services. Further, all public, FBO, and NGO facilities obtain their FP commodities
through the national level Medical Stores Department (MSD). A limited number of private, for-
profit clinics, pharmacies, and drug stores also provide some FP products and services, but data are
lacking on the numbers and distribution of such providers. Appendix A lists the planning partners
and implementers for the national FP program in the year 2009–2010.
An important step in implementing a reinvigorated FP program is to ensure that the process of
budgeting and financing for RH services and contraceptive commodities are understood by the
Council Health Management Team (CHMT). Requests from the CHMT are forwarded, usually in
November, through the Regional Medical Officer (RMO) to the Ministry of Finance and Economic
Affairs (MoFEA), which allocates governmental and Basket resources through the Medium-Term
Expenditures Framework (MTEF) in accordance with ceilings set through negotiations among the
MoHSW, MoFEA, President’s Office Planning Commission (POPC), and the Prime Minister’s
Office–Regional Administration and Local Government (PMO–RALG). At each level, additional
justification or clarification may be required for the budget requests, until a final approved budget is
submitted to Parliament in June. After approval by Parliament, the MTEF can dispense funds to the
CHMTs, usually on a quarterly basis. The process generally takes about nine months from initiation
until funds become available to support health services at the district and community levels.
The forecasting and quantification exercise, as well as the development of budgets and procurement
plans for contraceptive commodities, are done at the central level. Then, funds are sent to the MSD
for procurement and distribution of FP commodities to facilities. For funds that are administered
through the Basket fund, an additional level of approval or no objection from the World Bank is
required before ordering of contraceptive commodities. The standard time from when funds are
released from the MoFEA until the commodities arrive at MSD is six to nine months.
The FP program faces a number of challenges and constraints that must be addressed for effective
repositioning of FP to meet the country’s RH and development goals. Five program areas or
components are essential for implementing a successful FP program: a consistent and adequate

United Republic of Tanzania | National Family Planning Costed Implentantation Program
7
supply of contraceptive commodities; sufficient numbers of health providers who have the
necessary knowledge and the technical and client interactions skills to deliver FP services safely and
effectively; appropriately equipped facilities with a flexible array of service delivery modalities and
systems to meet the needs in different sociocultural contexts and levels of development in Tanzania’s
different regions; strong advocacy to increase visibility and support for the program and address the
knowledge-use gap among FP clients; and strong management systems and leadership to ensure
efficient and effective program implementation. The issues and challenges for each area have been
defined below based on a review of published literature and documents, through discussions with
the National Family Planning Working Group and through a series of key informant interviews (see
Appendix B for a summary report of these interviews).
Providing a choice of methods to meet the changing needs of clients throughout their reproductive
lives increases overall levels of contraceptive use and enables individuals and couples to meet their
reproductive goals. The method mix available in a program influences not only successful client
use and satisfaction, but also has implications for provider skills and the facilities and equipment
needed to deliver certain methods. All of these factors affect program cost and sustainability and,
in turn, the amount of contraceptive protection that can be provided with various levels of financial
support.
Maintaining an adequate supply of contraceptive commodities to meet clients’ needs, prevent stock-
outs and ensure contraceptive security is the most urgent issue facing the Tanzania’s FP program.
The inability to supply and sustain current users has considerable implications for expansion of
the program to meet the CPR targets of the One Plan. Other key strategies (HSSPIII and PHSDP)
recognize the importance of ensuring the availability of adequate contraceptive choices. General
strengthening of logistics systems planned in the PHSDP will benefit contraceptive security, but
additional investments are needed to ensure adequate forecasting, budgeting, and tracking of
supplies so that all contraceptive methods, especially those that are in greatest demand, are available
when and where clients need them.
Funding allocations through the MTEF are not adequate to meet contraceptive commodity
requirements because of competing priorities in the health sector. However, the government is
progressing well towards meeting the Abuja declaration target of 15 percent of the total national
budget to cover improvement in the health sector.
Furthermore, when requests for funding from the district level are prioritized and submitted for
funding by the district-level health management teams, FP falls well below other health service
priorities in some districts and is sometimes overlooked in these requests. As a result, stock-outs of
contraceptive commodities occur even when districts have returned unused funds to the Basket.
A key factor in ensuring contraceptive security, method-mix issues, has important implications
for cost as well as for client acceptance and satisfaction needed to sustain successful use.
Short-acting methods are the most prevalent contraceptives in the current method mix,
according to the 2004 DHS, which include pills, condoms, and, increasingly, injectable depot-
medroxyprogesterone (DMPA). These methods require regular resupply, hence successful use must
include access to a consistent supply of the product. Each ‘resupply’ visit to a service delivery
point (SDP) entails additional costs. Pills and condoms also require high levels of user adherence
and motivation, with inconsistent and incorrect use leading to method failures and high rates of
discontinuation.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
8
Condoms protect not only against unintended pregnancy but also against STIs, including HIV.
They have been widely promoted in HIV-prevention programs and, less often, as ‘dual protection’
against pregnancy and STIs/HIV. Their association with STI and HIV prevention, however, means
that for many couples, condoms are stigmatized as being associated with extramarital sex, and
therefore partners may resist using condoms for pregnancy prevention.
Long-acting methods give contraceptive protection for a year or more. They include intrauterine
devices (IUDs) and implants. These methods have higher initiation costs than short-acting methods,
but because they can be used without resupply for several years, they are often less expensive per year
of use. Initiation costs for these methods are higher because the costs of the commodities themselves
are higher. In addition, they require providers to have special training and skills for insertion and
removal as well as good counselling skills to ensure that clients can make informed choices about
these long-acting methods. Unlike short-acting methods, which can be discontinued simply by
the user stopping the method, discontinuation of IUDs and implants requires removal by a trained
provider.
Prevalence of IUD use in Tanzania is low, despite it being the most cost-effective form of reversible
contraception, having a good safety record, and providing highly effective contraceptive protection
for up to 10 years. Expanding the use of IUDs will require considerable attention to addressing myths
and misinformation about IUDs among both providers and clients. Hormone-releasing subdermal
implants provide safe, highly effective contraception and have been growing in popularity among
Tanzanian women.
Permanent methods of contraception (sterilization) include tubal ligation for women and vasectomy
for men. Worldwide, these two surgical methods account for the majority of contraceptive users
and are highly effective and safe when provided by trained personnel with appropriate attention
to infection control. Although the prevalence of permanent methods is low in Tanzania, the use of
tubal ligation is growing, especially for women who do not want more children, and a pilot program
to provide vasectomy in the Kigoma region is meeting with considerable success. Provision of
permanent methods is limited both by weaknesses in health facilities as well as by lack of provider
skills. Additionally, widespread rumours—for example, equating vasectomy with castration—
undermine acceptance of these highly effective methods. Because these methods limit future
childbearing, client education and counselling to ensure informed choice and informed consent are
essential parts of service provision. However, weaknesses exist in such client-provider interaction
skills. Expanded availability of permanent methods for those who do not want more children can
help Tanzania achieve its CPR targets, but this will require significant investments in capacity
building to ensure proficiency in surgical skills, counselling, and informed consent procedures.
Human resources are the most costly recurring expense in the health care system, with financial
resources needed not only to recruit and retain health care workers but also to ensure that they have
the knowledge, skills, and supervision to enable them to deliver safe, high-quality FP services.
For effective repositioning of FP to occur, health workers at all levels must see providing family
planning as their responsibility. National health-sector strategies (HSSPIII, HRHSP, and PHSDP)
include objectives to ensure sufficient numbers of health care providers at all levels of the system.
The NFPCIP will therefore focus on ensuring that health providers already in service, as well as
those in training and those to be hired, have the appropriate knowledge, skills, supervision, and
support to provide safe, effective, acceptable FP services.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
9
There is a critical shortage of skilled health care workers in Tanzania. Inadequate capacity for
planning, forecasting, and management of human resources are underlying factors affecting the
shortage. Distribution and retention of health care workers is also problematic. After almost a
decade-long employment freeze in the public sector during the Retrenchment Policy (1993–1999),
efforts to recruit health personnel have begun again. However, many posts, especially at rural
district levels, remain unfilled. Hardship living conditions in many districts, along with lack of
retention schemes, limited training opportunities, and overwhelming responsibilities, are major
factors undermining both recruitment and retention. According to a recent study, less than half of
Tanzania’s final-year medical students were willing to accept rural postings.
Low health worker productivity also contributes to the provider capacity challenge. Currently
a ‘pay-for-performance’ initiative is underway to enhance health worker productivity, but it has
no indicator for FP. Inclusion of an indicator for FP must avoid any target-setting that could be
construed as coercive.
Capacity building of providers to ensure essential skills in FP is in critical need of focused attention.
The national training strategy for FP is due for revision. Many current providers have not had their
FP knowledge and skills updated in several years, undermining the quality of care they provide. A
baseline survey of FP services in 2004–2005 found low levels of provider knowledge, clinical skills,
and counselling capability needed to provide quality FP services for both short- and long-acting
methods.
Provider biases and misinformation persist about certain methods and the appropriateness of FP
methods and services for selected categories of clients (youth, HIV-infected, etc.). The six Zonal
Training Centres, are charged with maintaining the knowledge and skills of current health providers.
Pre-service training for health professionals in some 116 health training institutions (public and
private sectors) must be strengthened.
Supervision needs strengthening, a fact recognized in the HRHSP, the HSSPIII, and the PHSDP.
Among the reasons for low health worker morale and poor retention rates are the lack of structured
and supportive supervision, including lack of written or oral feedback from supervision visits.
Investments through other program initiatives can strengthen supervision capacity in general.
Investments through the NFPCIP will help supervisors play more active roles in identifying
providers who need FP skills updates and in ensuring that those who are trained are applying their
updated knowledge and skills appropriately.
Access to a SDP is an essential component of FP. According to the Tanzania DHS 2004–2005,
more than 90 per cent of Tanzanians live within 10 kilometres of a health facility. The Tanzania
Baseline Survey conducted by the ACcess, Quality, and Use In REproductive health (ACQUIRE)
project in 2004–2005 found major deficiencies in the abilities of both clinic and hospital sites to
provide FP services, especially for long-acting and permanent methods (LAPMs). In areas where
the nearest health care provider is an FBO, the availability of FP services depends on the religious
beliefs and attitudes of the organization with regard to FP and contraception methods.
Infrastructure limits the types of FP services that can be provided in many health facilities. Higher-
level facilities, such as regional and district hospitals, are better equipped and supplied than are
health centres, and dispensaries. Some dispensaries and health centres, lack an on-site clean water
source and electricity, both essential for providing quality services, including infection control, for
LAPMs. Other infrastructure weaknesses include lack of private space for providing FP counselling

United Republic of Tanzania | National Family Planning Costed Implentantation Program
10
or services involving pelvic examinations and inadequate storage space for contraceptive supplies.
As with other areas, the major investments in strengthening infrastructure are being made through
the PHSDP and HSSPIII. The NFPCIP gives attention to ensuring that they are incorporated in
planning for upgrading of health infrastructure and equipment.
Considerable progress has been made to ensure the availability of equipment and supplies, such
as examining and surgical tables, lamps, sterile gloves, disposable needles, syringes, and containers
for sharps disposal, that are needed to provide some FP methods safely. However, consistent supply
in facilities, especially in community health facilities, needs to be further strengthened.
Utilization of services is influenced both by proximity and physical access to an SDP and by
client perceptions about the quality of care they are likely to receive. Factors influencing client
perceptions include the availability of counselling, information, and support provided to those
seeking FP services and particularly the consistent supply of contraceptive methods.
Efforts are underway to foster the integration of FP with other sexual reproductive health services,
such as FP and HIV/AIDS, FP and gender-based violence, FP in postnatal care (PNC), and FP in
postabortion care (PAC). However, many missed opportunities remain to integrate, promote, and
provide FP as part of other health services, such as with child immunization services. Integration of
services will help to reach new populations who may need FP and who must be reached to achieve
One Plan targets. Studies in other East African countries have shown that, even when providers of
these services lack the time or skills to provide direct services, they can assess the need for FP and refer
clients to an appropriate source.
Young people also need special attention, both in increasing their access to information, education,
and friendly services and in helping them to choose and use contraceptive methods effectively.
With adolescents constituting almost a third of Tanzania’s population, early sexual debut, and high
rates of pregnancy and childbearing among teenage girls, the needs for contraception are clear.
The MoHSW/Reproductive and Child Health Section (RCHS) has developed a national strategy
on adolescent RH that outlines key strategic objectives to enable adolescents to cope with their
growing up in this transition period. Despite having the strategy, many gaps still remain in terms
of fostering implementation of existing supportive policies and laws for young people to exercise
their sexual and reproductive rights; access friendly RH information, education, and services;
human resource capacity for providing services; and parent and community support towards young
people.
Referral systems need strengthening by ensuring that the referring provider has knowledge of
what FP services are available at referral centres, and has a mechanism to link clients to those
centres,. This has also been emphasized in the PHSDP and HSSPIII. Closer linkages with private,
NGO, and FBO facilities can be encouraged as part of the referral system.
In addition to clinic-based services, there are other options to deliver FP services. The decentralization
of responsibility for health care to the community level in Tanzania opens the door for expansion
of community-based services (CBS). Community-based services includes community-based
distribution (CBD) of short-acting methods now underway in a limited number of regions in
Tanzania, as well as making some methods available through accredited drug dispensing outlets
(ADDOs) and through pharmacies. Several issues and challenges must be addressed in considering
expansion of CBS, however. The CBD workers, as well as distributors in ADDOs and pharmacies,
need training and supervision to provide contraception, and this can entail considerable costs. Also,
CBD workers work on a voluntary basis; long-term retention of CBD workers requires that some
attention be given to nonmonetary rewards or noncoercive incentives.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
11
The basis of any strong program is a strong supportive policy framework, with high-level advocates
to maintain visibility and speak for the importance of the program. A supportive advocacy and
policy environment improves access to services and addresses normative barriers that restrict
provision of services. It mobilizes community and donor support for FP and is essential to secure
financing for the program, a crucial component of maintaining contraceptive security. It is essential
in promoting awareness of the benefits for FP and encouraging clients’ access to and use of services.
Strengthening capacity for advocacy called for in the PHSDP, and investments now underway to
expand information and communications technologies, will help to address the need for increased
advocacy for FP. The following paragraphs discuss the specific needs to be addressed through the
NFPCIP to strengthen advocacy for FP in Tanzania.
Sectoral reforms and decentralization, which began in the late 1990s and is still ongoing,
coincided with a slowing of the momentum achieved in the FP program in the mid- to late-
1990s. The sector-wide approach (SWAp) for health builds on the recommendations from the
1994 International Conference on Population and Development to integrate health services into
a comprehensive package that meets all client needs and reduces or eliminates vertical programs.
Because FP contributes to improvements in social and economic development, improvements in the
environment, and saving the lives of women, children, and adolescents, it is important to address FP
in a multisectoral approach.
Along with the SWAp, efforts to decentralize health care and promote community involvement
in and responsibility for health care were instituted. However, budget allocations still must be
increased for FP services at the district level. The MoHSW has developed a package of essential
interventions for empowering districts to include FP activities into Council Comprehensive Health
Plans (CCHP) guidelines.
Policy issues also directly affect the delivery of contraceptive methods and services. Although
policies set clear goals for making FP available to all who want and need services, without regard to
age, marital status, sex, or ability to pay, they are limited as to which categories of health personnel
are authorized to provide certain methods. These limitations must be reviewed according to the
local situation and needs and international norms and guidelines informed by recent research and
program evidence. Additionally, more effective dissemination of existing policies and guidelines, as
well as of updates and revisions, is needed so that all those implementing FP services are aware of
them.
Champions are important and needed to advocate for continued support and to promote use of
FP. There is a need to identify and recruit additional champions as well as orient and support their
activities at various levels.
Awareness levels of FP among Tanzanians are high. According to the 2004–2005 DHS, 96 percent
of all women and 97 percent of all men had heard of FP. However, knowledge does not equal
use of FP services. Obstacles that prevent adoption of FP among those who know about it include
actual or feared partner/spousal disapproval, myths, rumours and misinformation about FP and
specific methods, fears of side effects and health concerns, poor access to services and methods,
and concerns about costs. Public-sector facilities in Tanzania do not charge for FP methods and
services; however, poor infrastructure, shortage of skilled providers, and inconsistent availability of
contraceptive products all impede access to FP services by men, women, and adolescents.
In addition to those who fall within the traditional ‘unmet need’ category are all of those who remain
unaware of FP and its benefits or of their eligibility to access and use FP. These may include women

United Republic of Tanzania | National Family Planning Costed Implentantation Program
12
in remote rural areas, youth, men, or groups with special needs, such as HIV-infected persons.
Bridging the gap between current use and unmet need to reach the One Plan target of 60 percent
CPR by 2015 will require expanded efforts to increase demand for and use of FP in these groups.
Along with increasing demand is the need to ensure that services and commodities are available
to meet it. Demand-generation activities must be paced so that new demand for methods and
services can be met while current needs are being sustained. Planned investments in information
and communications technologies in HSSPIII and PHSDP will be of great benefit to activities that
aim to generate demand for FP.
Clear leadership and management responsibility and authority are essential for repositioning
FP overall and ensuring NFPCIP implementation. Increasing the number of RCHS staff and
management training is needed. The main challenges to achieving the goals of the NFPCIP are
that all of its elements must be fully funded and all recommended actions must be implemented
on schedule. For example, capacity building to ensure adequate human resources assumes sufficient
numbers of health care workers can be hired and trained. This will require full funding and
implementation of the PHSDP and HRHSP as the platform upon which the NFPCIP is built.
Achieving the goal also assumes there will be no unforeseen circumstances that will sidetrack
implementation and that political and traditional leaders at the national and community levels will
recognize and give priority to FP as a basic human right of their people.
Management systems and existing tools must be strengthened for successful repositioning of FP.
Among the challenges that must be addressed are ensuring a clearer understanding, especially at the
CHMT level, of how to prioritize FP in the budgeting process for the basket funding. Coordination
among all of the different agencies and organization involved in FP, sharing operational information,
and tracking implementation of the NFPCIP will require investments in strengthening both systems
and management skills to accomplish these essential tasks, including increased attention to public-
private partnerships for FP.
Monitoring and evaluation (M&E) systems also need strengthening, as recognized in HSSPIII. The
‘way forward’ calls for investments in developing a comprehensive M&E and research strategy for
the health and social welfare sector that is integrated with the health management information
system (HMIS). For the NFPCIP, this includes having adequately trained personnel to collect,
report, analyze, and use FP data for oversight of plan implementation and to recognize needs for and
make decisions about midcourse corrections to the NFPCIP.
Health sector reform, especially as noted in the HSSPIII, emphasizes public-/private-sector
partnerships. However, such partnerships in the FP services area are weak and must be strengthened.
The private, NGO, and FBO sectors can play an increased role in repositioning FP. Currently, the
government of Tanzania accounts for almost 70 percent of FP services in the country. Increasing the
role of the other sectors can help reallocate limited governmental resources to meet the needs of the
poorest of Tanzania’s citizens. It can also help generate demand by reaching new groups who are not
yet users of FP or who do not yet perceive a need for FP.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
13
National Family Planning Costed
Implementation Program
Purpose of the NFPCIP
Recognizing the need to reposition family planning in Tanzania, the MoHSW has developed the
NFPCIP. The development of the NFPCIP is guided by the vision and mission established in the
Reproductive and Child Health Policy Guidelines of 2003. Furthermore, the goal of the NFPCIP
is guided by the National Road Map Strategic Plan to Accelerate Reduction of Maternal, Newborn and
Child Deaths in Tanzania, 2008–2015 (One Plan) as well as by the HSSPIII. Both strategic plans
recognize family FP as essential to improving maternal, newborn, and child health. Although
the overall investments in the health sector called for in the HSSPIII, PHSDP, and HRHSP will
strengthen the foundation for FP, the specific aim of the NFPCIP is to identify the activities to
be implemented and additional resources that will be needed to make quality FP services more
accessible to and equitable for all of Tanzania’s people. Appendix C describes the process used to
develop the NFPCIP and provides a list of the individuals and organizations that participated in
this consultative, collaborative process.
The NFPCIP clearly defines priorities for strategic actions, delineates the activities and inputs needed
to achieve them, and estimates the costs associated with each as a basis for budgeting and mobilizing
resources required for implementation at different levels by organizations and institutions over the
2010–2015 period. In addition, the NFPCIP is intended to serve as a guide for development partners
and implementing agencies on areas of need to ensure the success of the national FP program.
More specifically, the NFPCIP will be used to:
Inform policy dialogue, planning and budgeting to strengthen FP as a priority area in the
National Development Agenda;
Prioritize FP program strategic actions and activities for implementation at different levels of
the health system;
Enable the MOHSW and other GoT sectors to understand the budgetary needs to implement
a FP program to reach projected targets, and to make projections for the future as new demand
for FP is generated;
Mobilize and sustain quality resources (human, financial, technical, commodities and equipment)
that are essential for achieving cost-effective and scaled-up services for FP; and
Provide benchmarks and indicators that can be used by GoT and development partners to
monitor and support the FP program;

United Republic of Tanzania | National Family Planning Costed Implentantation Program
14
A healthy and well-informed Tanzanian population with access to quality reproductive and child
health services that are acceptable, affordable, and sustainable and provided through efficient and
effective support systems.
Promote, facilitate and support in an integrated manner the provision of reproductive and child
health services to men, women, adolescents, and children in Tanzania.
Increase the CPR among women of reproductive age from 28 percent to 60 percent by 2015.
The denominator used for the CPR target is women of reproductive age and not married women
of reproductive age (MWRA). This is to take into consideration all women of reproductive age
regardless of their marital status. Furthermore, the CPR target includes all methods and not just
modern methods. According to the DHS 2004–2005, the CPR among MWRA for modern methods
is 20 percent and the CPR among MWRA for all methods is 26.4 percent, while the CPR for women
of reproductive age for all methods is 28 percent. The latter figure of 28 percent is thus used.
Although guidance is also provided by the HSSPIII, which has a goal CPR of 30 percent by 2015,
the higher CPR goal of 60 percent specified by the One Plan was chosen so that repositioning FP
can be addressed more aggressively and, as a result, will have greater potential impact on reducing
maternal and newborn mortality and improving child survival.
Furthermore, there is a wide degree of variation across regions in current CPR as well as considerations
of culture and context, such as the availability of infrastructure, human resources, service modalities,
and current demand. These factors increase the challenges to be addressed and the level of resources
that will be needed to reach the 60 percent CPR One Plan target by 2015. The regional variations
and the different scenarios for repositioning FP are discussed in more detail in the Analysis of
Demographic Determinants of Resource Requirements section.
The NFPCIP objectives reflect the five major program components that must be strengthened to
address the issues and challenges to reposition FP as a national priority for health and development.
Although all five components are needed for a thriving and effective program, emphasis will be given
to two areas to prioritize fulfilment of the increasing demand for FP services in the country. These
two areas include ensuring contraceptive security and strengthening integrated service delivery
of FP in all aspects of the health sector, including HIV/AIDS, immunization services, PNC, and
PAC.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
15

United Republic of Tanzania | National Family Planning Costed Implentantation Program
16
The nation’s demographic profile affects the ever-increasing need for resources for FP and hence is
taken into consideration to determine the resource requirements for the NFPCIP. Below are the
considerations and assumptions used for the NFPCIP to affect CPR projections and determine the
resources needed to meet the One Plan target of 60 percent CPR by 2015, assuming a growth rate
in CPR of five percentage points each year during 2010–2015. (Appendix D provides a definition
of the terms used in the NFPCIP and in the analysis):
The analysis that projects CPR and method-mix
targets for the NFPCIP is based on data from
the most recent DHS for Tanzania, conducted
in 2004–2005. To bring the CPR estimate to
2009, the growth in CPR has been assumed
to remained constant at 0.6 percentage points
annually since the last DHS, because that was
the rate of growth in CPR between 1999 and
2004–2005. A new DHS is currently ongoing
until late 2010. Findings from the new survey
may show this assumption to be incorrect because
of the loss in momentum in the FP program
discussed in the Introduction and the recent
and continuing stock-outs of contraceptives
discussed in the Issues and Challenges section.
If the growth in CPR is lower than has been
assumed, the challenges of meeting the One
Plan targets will be even greater.
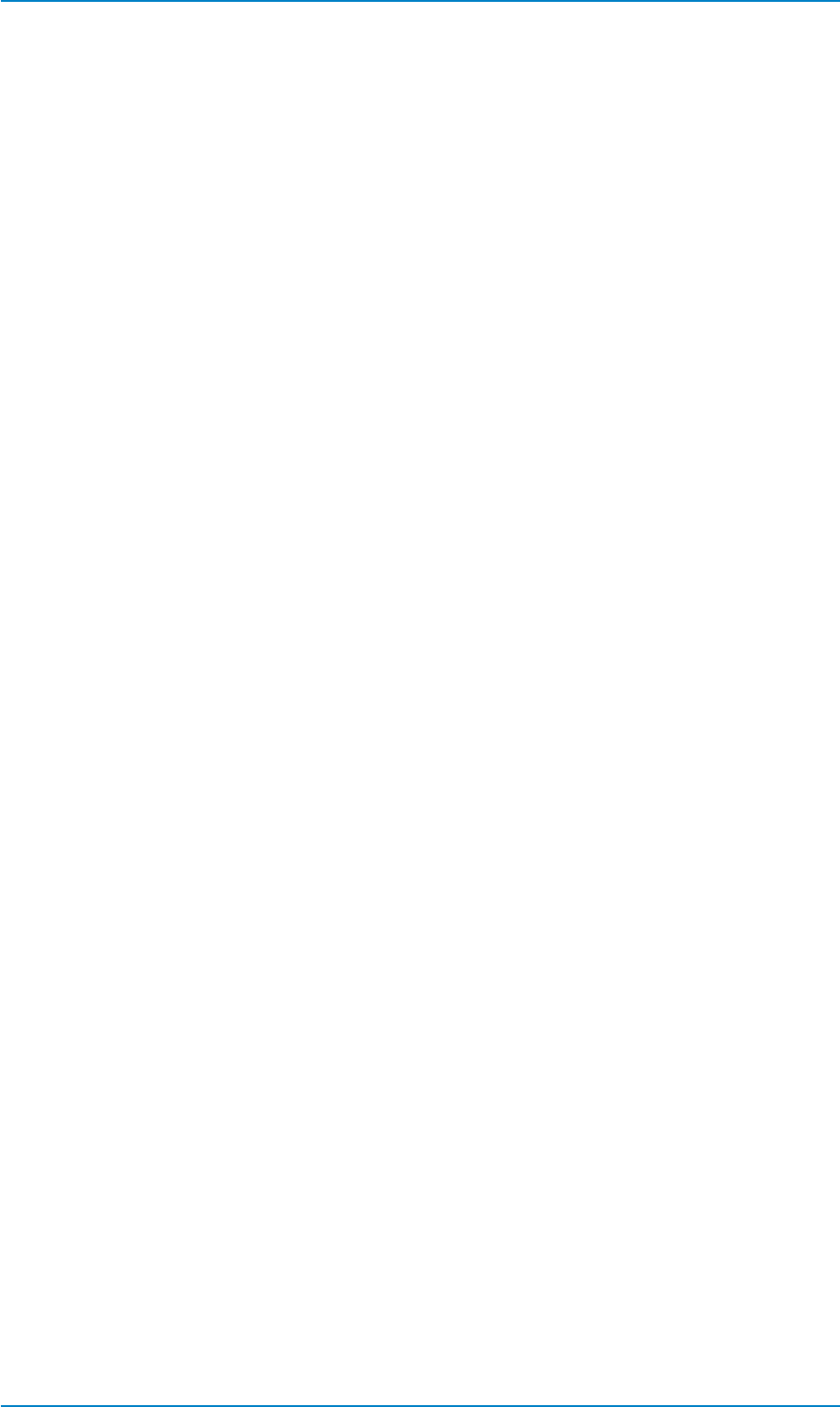
An important factor in these projections is that the total number of women of reproductive age
(WRA) expands each year. This is because of the age structure of Tanzania’s population (the
Population Pyramid). As shown in Table 1 (see Introduction), 47 percent of the population was
under 15 years of age in 2004–2005. All of the girls who will reach reproductive age between
now and 2015 have already been born, and each year an ever-increasing number of girls will reach
reproductive age. A number of women will also ‘age out’ of reproductive age each year, but because
of the population pyramid (Figure 1), that number will always be smaller than the number of girls
entering reproductive age. This growing denominator further stresses the FP program to deliver
more services to achieve the 60 percent CPR goal by 2015. Assuming a CPR of 28 percent in 2008,
there are 2.02 million current users of all methods of FP. To reach the One Plan target, taking into
account the growing denominator, the number of FP users must more than double, to a total of 5.23
million users by 2015.
0-4
5-9
15-19
10-14
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80+
Male Female
-10% -8%-6% -4%-2% 0% 2% 4% 6% 8% 10%
Age in Years
Percent of the population
Figure 1. Polpulation Pyramid for Tanzania

United Republic of Tanzania | National Family Planning Costed Implentantation Program
17
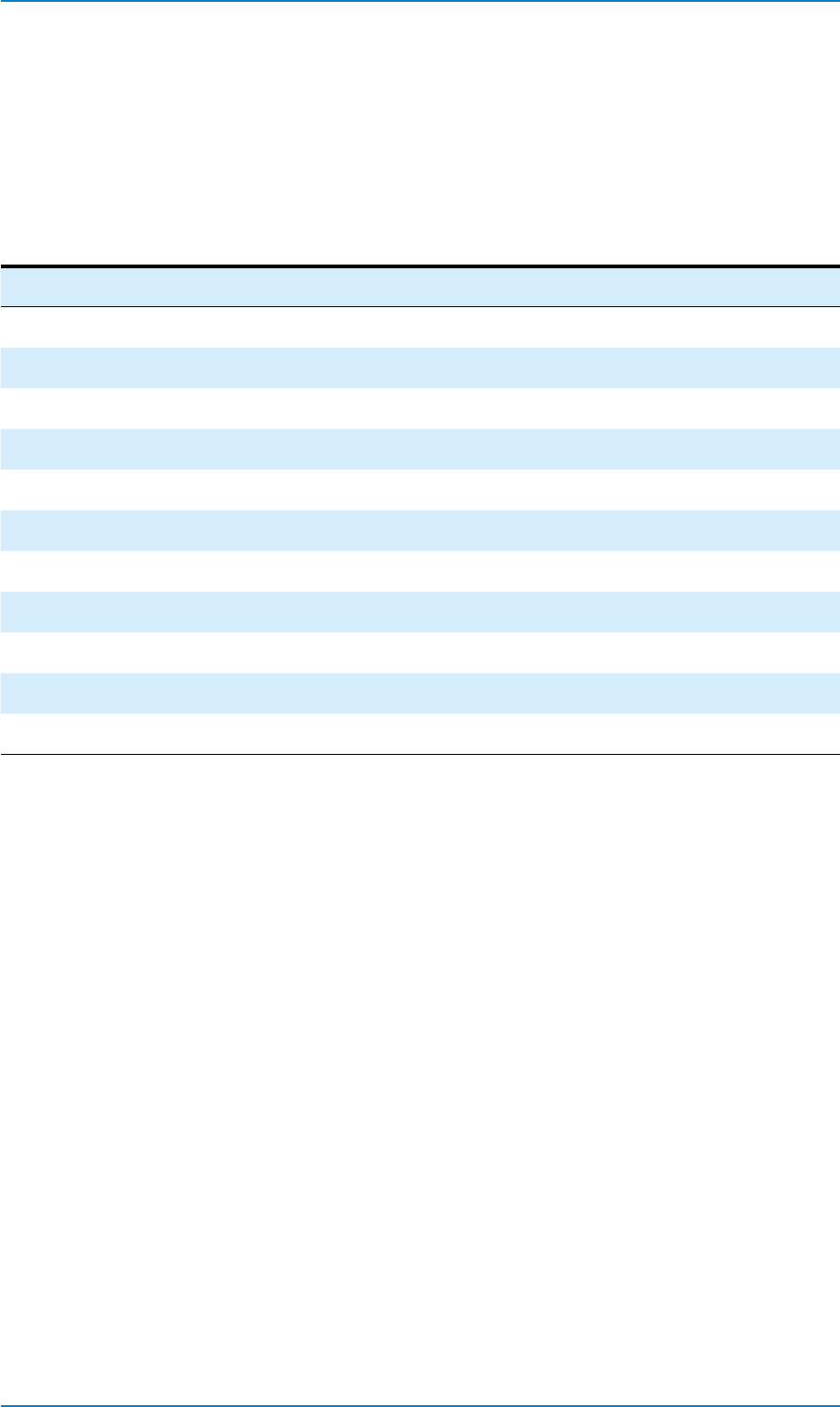
The map in Figure 2 shows the wide regional variations in CPR at the time of the last DHS. CPR
for all methods ranged from a low of 10.3 percent in Tabora region to a high of 49.5 percent in
Kilimanjaro region. Two thirds of the regions had a CPR of less than 40 percent. A number of
factors influence this variation in CPR, including availability of infrastructure and skilled providers,
social and cultural norms, and the relative level of priority given to FP by communities and local
governments. These factors, as well as the starting point of current CPR, will all influence whether
and how quickly each region can increase its CPR and contribute toward meeting the One Plan
target.
22%
35%
38%
30%
19%
35%
30%
26%
35%
26%
24%
17%
8%
13%
12%
8%
15%
9%
11%
17%
Modern Contraceptive
Prevalence 2004
29%
Source: TDHS 2004
Figure 2. Modern Contraceptive Prevalence by Region, 2005–2005
Table 3 shows that the mix of FP methods also varied by region at the time of the 2004–2005 DHS.
The Kilimanjaro region, with relatively stronger infrastructure and more highly trained providers,
for example, had the highest rates of use for LAPMs, whereas pills and condoms were more likely
to make up the majority of the method mix in regions with less well-equipped facilities and less-
skilled staff. It also shows the relatively high demand for injectables and the very low use of IUDs.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
18
Table 3. Contraceptive Method Mix by Region, DHS 2004–2005
Region
% Total
Population
Female
Sterilization Pill IUD Injectables Implant Condom LAPM
Kilimanjaro 0.062 10.2 6.8 1 17.2 1.6 1.5 0
Arusha 0.035 1.8 11.2 0.8 15.5 0.8 3 1.6
Mbeya 0.066 2 7 0 9.2 1 2.2 2
Dar es Salaam 0.07 3.7 11.6 0.9 13.7 1.5 3.4 0
Ruvuma 0.036 6.1 7.7 0 14.5 1.3 5.2 0
Tanga 0.053 1.8 6.3 0.5 15.5 0.9 4 0
Iringa 0.052 3.4 7.8 0 10.4 0 4.4 0.5
Morogoro 0.054 4.5 10.6 0 11.2 0.5 2.6 0.6
Lindi 0.026 3.5 18.3 0 6.1 0.4 1.8 0
Mtwara 0.034 2.2 13.6 0 9.2 0 0.9 0
Manyara 0.029 0.9 3.9 0 5.9 0 1.4 5.2
Dodoma 0.052 1 9.5 0 9.8 0 2 0
Coast (Pwani) 0.026 1.4 4.4 0 9.6 1.6 2.3 0
Kigoma 0.037 2.5 1.4 0.3 5.8 0 0.6 1
Singida 0.033 2.3 6.1 0.3 7.6 0 0.6 0
Rukwa 0.034 0.3 3.5 0.5 5.1 0 3.6 0
Kagera 0.059 3.4 3 0 7.5 0 1.1 0
Mara 0.042 1.8 1.1 0 6.7 0.3 0.6 0.3
Mwanza 0.08 2.2 2.2 0 3.2 0.3 0.6 0.7
Shinyanga 0.078 1.9 1.9 0 2.1 0.2 1.5 0
Tabora 0.043 1.2 0.5 0 4.5 0.3 1.3 0
Table 4 shows the projected total population for Tanzania in 2004 at 36 million, and the numbers
and percentages of the population residing in each region. It also shows the CPR, all methods, and
the total demand (CPR plus unmet need) in each region at the time of the DHS (2004–2005), with
an overall CPR of 28 percent. This table groups the regions into five strata based on the CPR. For
each stratum, it shows at the time of the last DHS the relative contribution that each stratum made
toward achieving a national CPR of 60 percent. The table also shows the stratum-specific CPR that
must be reached by 2015 to achieve the One Plan target. For example, Stratum 1 shows Kilimanjaro
and Arusha having the highest CPRs in 2004–2005. These two regions account for 9.7 percent of
Tanzania’s total population. For the country to reach 60 percent CPR overall, the regions in Stratum
1 will need to reach a CPR of 72 percent by 2015. The stratum with the lowest CPR, and with
almost a quarter of Tanzania’s population, will need to increase its CPR from around 11 percent
in 2004–2005 to 49 percent by 2015 for the country to reach its One Plan target. All regions will
need to increase demand to reach their targets, but meeting the current total demand in each region
would make a significant contribution to reaching the targets.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
19
Table 4. Population, CPR (2004–2005), and Total Demand with Regional Stratication and CPR Targets to Reach One
Plan Target
Region
2004–2005 DHS Stratum Analysis
Projected
population
CPR, all
methods
Total
demand
% Total
Population
2015 CPR
Target
% Total
Population
Relative
Contribution
Kilimanjaro 2,228,526 49.50% 69.60% 6.20%
72.00% 9.70% 0.07
Arusha 1,247,982 48.60% 65.50% 3.50%
Mbeya 2,369,368 45.10% 57.50% 6.60%
68.00% 22.50% 0.153
Dar es Salaam 2,522,531 44.60% 59.60% 7.00%
Ruvuma 1,280,113 41.60% 59.60% 3.60%
Tanga 1,922,318 40.20% 60.60% 5.30%
Iringa 1,871,754 35.10% 54.80% 5.20%
62.00% 27.20% 0.169
Morogoro 1,928,864 34.60% 50.20% 5.40%
Lindi 939,928 33.50% 55.20% 2.60%
Mtwara 1,225,136 26.80% 51.30% 3.40%
Manyara 1,041,894 26.50% 54.50% 2.90%
Dodoma 1,861,085 23.80% 52.20% 5.20%
Coast (Pwani) 935,906 22.20% 46.80% 2.60%
Kigoma 1,331,265 19.80% 52.80% 3.70%
55.00% 16.30% 0.09
Singida 1,204,090 18.30% 43.50% 3.30%
Rukwa 1,231,549 18.10% 35.50% 3.40%
Kagera 2,108,853 15.70% 38.80% 5.90%
Mara 1,530,609 13.00% 42.40% 4.20%
49.00% 24.30% 0.119
Mwanza 2,882,978 11.00% 38.90% 8.00%
Shinyanga 2,794,746 10.90% 42.60% 7.80%
Tabora 1,561,744 10.30% 34.80% 4.30%
Total 36,021,239 28.10% Total CPR 60.00%
Table 5 shows the annual CPR, all methods, that each region will need to reach to achieve the One
Plan target of 60 percent CPR by 2015. It assumes a 0.6 percentage point growth in CPR each year
since the last DHS. These projections serve as the basis for estimating the commodities and other
inputs that will be required to deliver the projected volume and mix of FP services. Although not
all of the regions will reach the One Plan target by 2015, the nation as a whole would meet the 60
percent target at this growth rate in CPR. In all, 13 regions will meet or exceed 60 percent CPR at
this rate of growth; the remainder will achieve lower CPRs.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
20
Table 5. Growth in CPR, Assuming a 0.6 percent Increase from 2004 to 2009 and Reaching National Target in 2015
Region
2004–2005 DHS PROJECTIONS
CPR all
method
% Total
Population
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
Kilimanjaro 49.50% 6.20% 50% 51% 51% 52% 53% 56% 59% 62% 66% 69% 72%
Arusha 48.60% 3.50% 49% 50% 50% 51% 52% 55% 58% 62% 65% 69% 72%
Mbeya 45.10% 6.60% 46% 46% 47% 48% 48% 51% 55% 58% 61% 65% 68%
Dar es Salaam 44.60% 7.00% 45% 46% 46% 47% 48% 51% 54% 58% 61% 65% 68%
Ruvuma 41.60% 3.60% 42% 43% 43% 44% 45% 49% 52% 56% 60% 64% 68%
Tanga 40.20% 5.30% 41% 41% 42% 43% 43% 47% 51% 56% 60% 64% 68%
Iringa 35.10% 5.20% 36% 36% 37% 38% 38% 42% 46% 50% 54% 58% 62%
Morogoro 34.60% 5.40% 35% 36% 36% 37% 38% 42% 46% 50% 54% 58% 62%
Lindi 33.50% 2.60% 34% 35% 35% 36% 37% 41% 45% 49% 54% 58% 62%
Mtwara 26.80% 3.40% 27% 28% 29% 29% 30% 35% 41% 46% 51% 57% 62%
Manyara 26.50% 2.90% 27% 28% 28% 29% 30% 35% 40% 46% 51% 57% 62%
Dodoma 23.80% 5.20% 24% 25% 26% 26% 27% 33% 39% 44% 50% 56% 62%
Coast (Pwani) 22.20% 2.60% 23% 23% 24% 25% 25% 31% 37% 44% 50% 56% 62%
Kigoma 19.80% 3.70% 20% 21% 22% 22% 23% 28% 34% 39% 44% 50% 55%
Singida 18.30% 3.30% 19% 20% 20% 21% 21% 27% 33% 38% 44% 49% 55%
Rukwa 18.10% 3.40% 19% 19% 20% 21% 21% 27% 32% 38% 44% 49% 55%
Kagera 15.70% 5.90% 16% 17% 18% 18% 19% 25% 31% 37% 43% 49% 55%
Mara 13.00% 4.20% 14% 14% 15% 15% 16% 22% 27% 33% 38% 44% 49%
Mwanza 11.00% 8.00% 12% 12% 13% 13% 14% 20% 26% 32% 37% 43% 49%
Shinyanga 10.90% 7.80% 12% 12% 13% 13% 14% 20% 26% 31% 37% 43% 49%
Tabora 10.30% 4.30% 11% 12% 12% 13% 13% 19% 25% 31% 37% 43% 49%
National 28.1% 28.7 29.3 29.9 30.5 31.1 35.9 40.7 45.6 50.4 55.2 60
The next table, Table 6, sets the method-mix targets to be achieved in each region by 2015 to
meet the One Plan target. The analysis in this table, an important step in estimating the volume
of contraceptive commodities that must be available each year, is based on the use of each method
reported in the last DHS and on recent expansion in availability and demand for some methods.
The targets are shown are the percentage levels that each method is expected to reach in each region,
totalling to 100 percent in each region. The projections in this table take into account a variety of
contextual factors, including sociocultural considerations, availability of infrastructure, and provider
capacity, that are likely to influence provision and acceptance of each method. These targets also
take into consideration the recommendations of the National Family Planning Working Group to
shift use, wherever feasible, from less effective to more effective methods while maintaining the
widest possible range of method choices. For example, targets assume a shift of some users from
traditional to modern methods. Within temporary methods, some users are shifted from those
methods requiring high levels of personal adherence (pills and condoms) to injectables. An overall
shift to LAPMs is also assumed, especially in regions with better infrastructure and more highly
skilled providers.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
21
Table 6. Contraceptive Method-Mix Targets, 2015, by Region, Based on Contextual Factors
Region
Female
Sterilization Pills IUD Injectables Implant Condoms Traditional
Kilimanjaro 16.0% 7.0% 9.0% 50.0% 10.0% 3.0% 5.0%
Arusha 3.0% 18.0% 3.0% 50.0% 9.0% 7.0% 10.0%
Mbeya 3.6% 14.0% 2.4% 34.0% 6.0% 5.0% 35.0%
Dar es Salaam 6.0% 22.0% 4.0% 40.0% 15.0% 8.0% 5.0%
Ruvuma 10.0% 14.0% 2.5% 40.0% 12.5% 13.0% 8.0%
Tanga 3.0% 23.0% 2.4% 45.0% 6.6% 10.0% 10.0%
Iringa 6.3% 25.0% 2.4% 35.0% 3.3% 13.0% 15.0%
Morogoro 8.5% 22.0% 3.0% 45.0% 8.5% 8.0% 5.0%
Lindi 6.6% 37.0% 3.6% 35.0% 7.8% 6.0% 4.0%
Mtwara 4.3% 40.0% 2.4% 45.0% 5.3% 3.0% 0.0%
Manyara 2.0% 30.0% 1.2% 30.0% 2.8% 6.0% 28.0%
Dodoma 2.2% 20.0% 1.6% 60.0% 4.2% 8.0% 4.0%
Coast (Pwani) 4.0% 10.0% 4.0% 55.0% 12.0% 10.0% 5.0%
Kigoma 5.7% 9.0% 4.0% 38.0% 10.3% 3.0% 30.0%
Singida 5.2% 15.0% 4.0% 60.0% 10.8% 3.0% 2.0%
Rukwa 2.3% 22.0% 1.4% 35.0% 3.0% 21.0% 15.3%
Kagera 7.8% 8.0% 6.0% 53.0% 16.2% 7.0% 2.0%
Mara 4.7% 5.0% 4.0% 60.0% 11.3% 5.0% 10.0%
Mwanza 6.5% 20.0% 6.0% 40.0% 17.5% 6.0% 4.0%
Shinyanga 6.0% 16.0% 6.0% 30.0% 18.0% 16.0% 8.0%
Tabora 4.0% 5.0% 4.0% 56.0% 12.0% 14.0% 5.0%
National 5.9% 17.5% 4.0% 44.0% 10.4% 8.4% 9.8%
Based on the method-mix targets in Table 6, Table 7 projects the annual rate of growth in each
method that will be required in all regions, starting in 2010 and reaching the One Plan target of 60
percent CPR by 2015. This table is used to project the absolute volume of commodities that will be
required each year to achieve the One Plan target.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
22
Table 7. Annual Rate of Growth by Contraceptive Method, by Region, 2010–2015, to Achieve One Plan CPR Target
Method mix targets @ 60% CPR in 2015
Region 2010 2011 2012 2013 2014 2015
% Pop
Yrs to target
Fster
Pill
IUD
Inject
Implant
Cond
Trad
Fster
Pill
IUD
Inject
Implant
Cond
Trad
Fster
Pill
IUD
Inject
Implant
Cond
Trad
Fster
Pill
IUD
Inject
Implant
Cond
Trad
Fster
Pill
IUD
Inject
Implant
Cond
Trad
Fster
Pill
IUD
Inject
Implant
Cond
Trad
Kilimanjaro 0.062 6 0.11 0.07 0.02 0.22 0.03 0.02 0.10 0.11 0.07 0.03 0.25 0.04 0.02 0.08 0.11 0.06 0.04 0.27 0.04 0.02 0.07 0.11 0.06 0.05 0.30 0.05 0.02 0.06 0.11 0.05 0.06 0.33 0.06 0.02 0.05 0.12 0.05 0.06 0.36 0.07 0.02 0.04
Arusha 0.035 6 0.02 0.13 0.01 0.22 0.02 0.04 0.11 0.02 0.13 0.01 0.24 0.03 0.04 0.10 0.02 0.13 0.02 0.27 0.04 0.04 0.10 0.02 0.13 0.02 0.30 0.05 0.05 0.09 0.02 0.13 0.02 0.33 0.06 0.05 0.08 0.02 0.13 0.02 0.36 0.06 0.05 0.07
Mbeya 0.066 6 0.02 0.09 0.00 0.13 0.02 0.03 0.23 0.02 0.09 0.01 0.15 0.02 0.03 0.23 0.02 0.09 0.01 0.17 0.03 0.03 0.23 0.02 0.09 0.01 0.19 0.03 0.03 0.23 0.02 0.09 0.01 0.21 0.04 0.03 0.24 0.02 0.10 0.02 0.23 0.04 0.03 0.24
Dar es Salaam 0.070 6 0.04 0.13 0.01 0.17 0.03 0.04 0.09 0.04 0.13 0.02 0.19 0.04 0.04 0.08 0.04 0.14 0.02 0.21 0.06 0.05 0.07 0.04 0.14 0.02 0.23 0.07 0.05 0.06 0.04 0.15 0.02 0.25 0.09 0.05 0.05 0.04 0.15 0.03 0.27 0.10 0.05 0.03
Ruvuma 0.036 6 0.07 0.09 0.00 0.18 0.03 0.06 0.07 0.07 0.09 0.01 0.20 0.04 0.07 0.06 0.07 0.09 0.01 0.21 0.05 0.07 0.06 0.07 0.09 0.01 0.23 0.06 0.08 0.06 0.07 0.09 0.01 0.25 0.07 0.08 0.06 0.07 0.10 0.02 0.27 0.09 0.09 0.05
Tanga 0.053 6 0.02 0.08 0.01 0.19 0.02 0.05 0.11 0.02 0.10 0.01 0.21 0.02 0.05 0.10 0.02 0.11 0.01 0.24 0.03 0.06 0.09 0.02 0.13 0.01 0.26 0.03 0.06 0.09 0.02 0.14 0.01 0.28 0.04 0.06 0.08 0.02 0.16 0.02 0.31 0.04 0.07 0.07
Iringa 0.052 6 0.04 0.10 0.00 0.13 0.00 0.05 0.10 0.04 0.11 0.01 0.15 0.01 0.06 0.09 0.04 0.12 0.01 0.17 0.01 0.06 0.09 0.04 0.13 0.01 0.18 0.01 0.07 0.09 0.04 0.14 0.01 0.20 0.02 0.08 0.09 0.04 0.16 0.01 0.22 0.02 0.08 0.09
Morogoro 0.054 6 0.05 0.12 0.00 0.15 0.01 0.03 0.04 0.05 0.13 0.01 0.18 0.02 0.04 0.04 0.05 0.13 0.01 0.20 0.03 0.04 0.04 0.05 0.13 0.01 0.23 0.04 0.04 0.03 0.05 0.13
0.02 0.25 0.04 0.05 0.03 0.05 0.14 0.02 0.28 0.05 0.05 0.03
Lindi 0.026 6 0.04 0.22 0.00 0.10 0.01 0.02 0.02 0.04 0.22 0.01 0.12 0.02 0.03 0.02 0.04 0.22 0.01 0.14 0.03 0.03 0.02 0.04 0.22 0.01 0.17 0.03 0.03 0.02 0.04 0.23 0.02 0.19 0.04 0.03 0.02 0.04 0.23 0.02 0.22 0.05 0.04 0.02
Mtwara 0.034 6 0.03 0.17 0.00 0.13 0.01 0.01 0.00 0.03 0.19 0.01 0.16 0.01 0.01 0.00 0.03 0.20 0.01 0.19 0.02 0.01 0.00 0.03 0.22 0.01 0.22 0.02 0.02 0.00 0.03 0.23 0.01 0.25 0.03 0.02 0.00 0.03 0.25 0.01 0.28 0.03 0.02 0.00
Manyara 0.029 6 0.01 0.07 0.00 0.09 0.00 0.02 0.15 0.01 0.09 0.00 0.11 0.01 0.02 0.16 0.01 0.12 0.00 0.13 0.01 0.03 0.16 0.01 0.14 0.01 0.15 0.01 0.03 0.16 0.01 0.16 0.01 0.17 0.01 0.03 0.17 0.01 0.19 0.01 0.19 0.02 0.04 0.17
Dodoma 0.052 6 0.01 0.11 0.00 0.15 0.00 0.03 0.02 0.01 0.11 0.00 0.20 0.01 0.03 0.02 0.01 0.12 0.01 0.24 0.01 0.04 0.02 0.01 0.12 0.01 0.28 0.02 0.04 0.02 0.01 0.12 0.01 0.33 0.02 0.05 0.02 0.01 0.12 0.01 0.37 0.03 0.05 0.02
Coast (Pwani) 0.026 6 0.02 0.05 0.00 0.15 0.03 0.03 0.03 0.02 0.05 0.01 0.19 0.04 0.04 0.03 0.02 0.06 0.01 0.22 0.05 0.04 0.03 0.02 0.06 0.02 0.26 0.06 0.05 0.03 0.02 0.06 0.02 0.30 0.07 0.06 0.03 0.02 0.06 0.02 0.34 0.07 0.06 0.03
Kigoma 0.037 6 0.03 0.02 0.01 0.09 0.01 0.01 0.11 0.03 0.03 0.01 0.12 0.02 0.01 0.12 0.03 0.03 0.01 0.14 0.03 0.01 0.13 0.03 0.04 0.02 0.16 0.04 0.01 0.14 0.03 0.04 0.02 0.19 0.05 0.01 0.15 0.03 0.05 0.02 0.21 0.06 0.02 0.17
Singida 0.033 6 0.03 0.08 0.01 0.13 0.01 0.01 0.01 0.03 0.08 0.01 0.17 0.02 0.01 0.01 0.03 0.08 0.01 0.21 0.03 0.01 0.01 0.03 0.08 0.02 0.25 0.04 0.01 0.01 0.03 0.08 0.02 0.29 0.05 0.01 0.01 0.03 0.08 0.02 0.33 0.06 0.02 0.01
Rukwa 0.034 6 0.01 0.06 0.01 0.08 0.00 0.06 0.06 0.01 0.07 0.01 0.11 0.01 0.07 0.06 0.01 0.08 0.01 0.13 0.01 0.08 0.07 0.01 0.09 0.01 0.15 0.01 0.09 0.07 0.01 0.11 0.01 0.17 0.01 0.10 0.08 0.01 0.12 0.01 0.19 0.02 0.12 0.08
Kagera 0.059 6 0.04 0.04 0.01 0.12 0.01 0.02 0.01 0.04 0.04 0.01 0.16 0.03 0.02 0.01 0.04 0.04 0.02 0.19 0.04 0.03 0.01 0.04 0.04 0.02 0.22
0.06 0.03 0.01 0.04 0.04 0.03 0.26 0.07 0.03 0.01 0.04 0.04 0.03 0.29 0.09 0.04 0.01
Mara 0.042 6 0.02 0.02 0.00 0.12 0.01 0.01 0.03 0.02 0.02 0.01 0.15 0.02 0.01 0.04 0.02 0.02 0.01 0.19 0.03 0.02 0.04 0.02 0.02 0.01 0.22 0.04 0.02 0.04 0.02 0.02 0.02 0.26 0.05 0.02 0.05 0.02 0.02 0.02 0.29 0.06 0.02 0.05
Mwanza 0.080 6 0.03 0.04 0.01 0.07 0.02 0.01 0.02 0.03 0.05 0.01 0.10 0.03 0.02 0.02 0.03 0.06 0.01 0.12 0.05 0.02 0.02 0.03 0.08 0.02 0.15 0.06 0.02 0.02 0.03 0.09 0.02 0.17 0.07 0.03 0.02 0.03 0.10 0.03 0.20 0.09 0.03 0.02
Shinyanga 0.078 6 0.03 0.04 0.01 0.05 0.02 0.03 0.03 0.03 0.05 0.01 0.07 0.03 0.04 0.03 0.03 0.05 0.01 0.09 0.05 0.05 0.03 0.03 0.06 0.02 0.11 0.06 0.06 0.03 0.03 0.07 0.02 0.13 0.07 0.07 0.04 0.03 0.08 0.03 0.15 0.09 0.08 0.04
T
abora 0.043 6 0.02 0.01 0.00 0.10 0.01 0.03 0.02 0.02 0.01 0.01 0.13 0.02 0.04 0.02 0.02 0.02 0.01 0.17 0.03 0.04 0.02 0.02 0.02 0.01 0.20 0.04 0.05 0.02 0.02 0.02 0.02 0.24 0.05 0.06 0.02 0.02 0.02 0.02 0.27 0.06 0.07 0.02
National 0.03 0.08 0.01 0.13 0.02 0.03 0.07 0.03 0.08 0.01 0.16 0.02 0.03 0.06 0.04 0.09 0.01 0.18 0.03 0.04 0.06 0.04 0.10 0.02 0.21 0.04 0.04 0.06 0.04 0.10 0.02 0.24 0.05 0.05 0.06 0.04 0.11 0.02 0.26 0.06 0.05 0.06
Method mix 9.7% 21.8% 1.7% 36.5% 4.2% 8.0% 18.2% 8.6% 20.6% 2.3% 38.7% 6.0% 8.1% 15.8% 7.7% 19.7% 2.8% 40.4% 7.3% 8.1% 13.9% 7.1% 18.9% 3.3% 41.8% 8.4% 8.2% 12.4% 6.5% 18.3% 3.6% 43.0% 9.3% 8.2% 11.1% 6.0% 17.8% 3.9% 43.9% 10.1% 8.2% 10.1%
Fster: Female Sterilization
Inject: Injectables
Cond: Condoms
Trad: Traditional methods

United Republic of Tanzania | National Family Planning Costed Implentantation Program
23
Tanzania’s FP program must be revitalized to achieve an annual growth rate in CPR of 5 percentage
points or to even return to a growth rate of 1.5 percentage points. The NFPCIP has five SAAs to
revitalize and reposition FP to obtain an overall increase in CPR consistent with the One Plan target
of 60%. Each SAA has a set of strategic actions that are broken down into the various activities
or steps needed for implementation, and the activities are further specified with required inputs
that form the basis for estimating the cost. The strategic actions and activities address the issues
and challenges discussed previously to ensure that FP considerations and resources are integrated
with other ongoing health sector strategic programs, such as the HSSPIII, PHSDP, and HRHSP.
As noted elsewhere, the activities and their costs included here are aimed specifically at what is
needed to address, elevate, and include FP as a coequal program along with other health sector
program initiatives. These costs therefore do not duplicate investments in other strategic health
programs. Cost estimates for implementing activities at the District level have not been included
in the NFPCIP. These have been included in a complementary document to guide District planners
to budget essential interventions that will contribute to the NFPCIP targets and thus should be
included in the CCHPs. Furthermore, the government contributions to the NFPCIP, including
salaries for human resources and infrastructure (equipment, furniture, supplies, electricity, and
water supplies), can range from 40 to 60 percent of the total budgetary estimates. These estimates
have not been included in the NFPCIP.
The following tables describe the activities for each SAA, and the timeframe and process for
implementation are indicated. A detailed breakdown of factors is shown as the basis for estimating
the costs for each activity. Finally, the success indicator for monitoring Plan implementation is
shown for each SAA. More detail for each SAA is provided in Appendix E.
Given the need to fulfil increasing demand for FP services in the country, two areas have been identified
as the key priorities for implementation and funding of the NFPCIP: ensuring contraceptive security
and enhancing service delivery and capacity building, in particular, strengthening integrated service
delivery of FP in all aspects of the health sector, including HIV/AIDS, immunization services, PNC,
and PAC. As such, contraceptive commodities represent 91 percent of the total NFPCIP budget.
In the beginning stages, focus will be on meeting demand; in subsequent years, efforts will be
enhanced to generate and sustain demand for FP to meet the One Plan target.
This SAA refers to expanded availability and choices of safe, effective, acceptable and affordable
contraceptive methods. It addresses contraceptive logistics and security, ensuring that supplies
of all contraceptive commodities are adequate to meet the needs and preferences of family planning
clients.
Based on the method-mix targets to be achieved in each region by 2015 to meet the One Plan target
(see Table 7), the number of users to be reached is an estimated 5.23 million WRA at an annual cost
ranging from Tshs 16 billion in FY 2010–2011 to 25 billion in FY 2015–2016.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
24
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
Strategic Action 1. Ensure adequate supply of contraceptive methods at all levels
1(a) Ensure sufficient donor and MoFEA funds
to cover all public-sector contraceptive
commodity needs
Years 1–6 Funding requests match
resource needs
119,997,745,046
1(b) Establish a forum of regular monthly
meetings with MSD, RCHS, PSU, World
Bank, and Supplies Unit to discuss status of
ongoing procurement, identify bottlenecks,
and stock situation countrywide and by zone
Year 1 # meetings held; evidence
that issues identified are
dealt with before next
meeting
54,952,500
1(c) Streamline forecasting, procurement,
distribution, use monitoring, and reporting
Year 1 Increased budget
allocation for
contraceptives; reduced
stock-outs
81,940,500
1(d) Develop an automated system to capture
facility-level logistics data and make
available to district, regional, and central
decision makers (may involve use of
cellphone technology)
Year 1: develop
Years 2–6:
implement
Increased availability of
accurate data
1,005,226,000
1(e) Conduct supportive supervisions to MSD
HQ, Zonal MSD, and health facilities for
contraceptive commodities (4 supervisions
per quarter); supervisory team to include 2
RCHS, 1 Zonal RCHCO, 1 RCHCO, and
DRCHCO
Years 1–2:
register Years
3–6: distribute
Reduce % unmet needs;
increase CPR
189,360,000
Contraceptive Security Total (in Tshs): 121,329,224,046
DRCHCo = district reproductive and child health coordinator; MSD = Medical Stores Department; PSU = Program
Support Unit; RCHCo = district reproductive and child health coordinator; RCHS = Reproductive and Child Health
Section.
This SAA refers to capacity building of providers to deliver and support the safe, effective
use of FP methods and services. It addresses the capacity of the people who deliver FP services.
Capacity-building considerations include the numbers, categories, attitudes, skills, supervision, and
remuneration of service personnel at all levels and in all sectors.
STRATEGIC ACTIVITIES TIMEFRAME SUCCESS INDICATOR
COST
(FY 2010–2016)
Strategic Action 1. Increase availability and improve distribution of FP service providers
1(a) Develop, implement computerized
inventory of staff by facility to identify
gaps and ensure equitable distribution
Years 1–6 On-line facility specific
staff inventory available
and updated annually
0
1
Strategic Action 2. Implement task shifting to all levels of the health system
2(a) Identify opportunities for task shifting
by cadre of health services provider for
expanded and integrated FP provision
Year 1 Report on potential for
task shifting and necessary
changes
22,250,500
2(b) Consultations with professional
associations and registrars (MAT, TAMA,
AGOTA, PAT, pharmacists, lab associates)
on how best to implement evidence-based
task shifting for FP provision
Year 2 Report on potential for
task shifting and necessary
changes
14,310,000

United Republic of Tanzania | National Family Planning Costed Implentantation Program
25
STRATEGIC ACTIVITIES TIMEFRAME SUCCESS INDICATOR
COST
(FY 2010–2016)
2(c) Consult with relevant authorities on
recommendations for policy amendments
Year 3 Recommendations
developed for task shifting
14,310,000
2(d) Produce and disseminate policy
amendments nationwide
Year 3 Policy amendments made 4,225,000
Strategic Action 3. Improve provider capacity to deliver FP services
3(a) Update national FP training strategy Year 1 Updated strategy in place 24,288,750
3(b) Identify and update an inventory of
national FP trainers
Years 1, 5 Inventory of FP trainers
available
200,000
3(c) Print additional copies of the updated FP
procedures manual (3,000) and training
curricula (500–Module I; 300–Module II;
100–Module III)
Year 2 # materials produced by
type
7,950,000
3(d) Disseminate updated FP procedures
manual and training curricula
Years 1–2 # trainers oriented with
the new manual and
curricula
102,060,750
3(e) Update preservice curricula with up-to-
date and comprehensive FP content
Years 1–2 Updated pre-service
curricula available
32,456,500
3(f) Train 80 tutors per year in pre-service
training institutions on FP curricula
Years 2–4 # tutors trained in new
curricula
113,048,000
3(g) Review job aids on client-provider
interaction. Print 5,000 job aids for
client-provider interaction.
Year 1 Final job aid produced 54,876,000
3(h) Disseminate/orient providers on client-
provider interaction.
Year 1 # copies of toolkit produced 173,702,500
3(i) Increase the pool of zonal FP trainers Years 2–4 # trainers produced 316,434,000
3(j) Conduct CTU in-service training using
updated curricula and job aids
Years 1–6 # trainings conducted 3,624,672,000
3(k) Conduct training on short- and long-
acting methods
Years 1–2 # trainings conducted 483,115,0003
3(l) Conduct training on permanent methods Years 1–2 # trainings conducted 393,140,0003
Strategic Action 4. Retain retiring and rehire retired health workers
4(a) Identify retiring and retired health
workers, especially those with FP
experience, and rehire
Years 1–6 # of retiring and retired
health workers retained
0
2
4(b) Identify training needs and develop
training plan for rehired workers
Years 1–6 Training needs
documented, training plan
developed
0
2
4(c) Implement training as needed for retired
health workers and allocate as needed
Years 1–6 Trainings held, # trainees
reached, increased # of SP
providing FP services
0
2
Strategic Action 5. Include non-coercive FP indicators in pay-for-performance initiative
5(a) Develop noncoercive FP indicator in pay-
for-performance initiative
Year 1 Report on-job satisfaction
survey
0
5(b) Ensure inclusion of FP indicator in the
benefits package
Years 2–6 Benefit package system
established/reviewed
5,617,000
Strategic Action 6. Build capacity for FP advocacy at regional and district levels
2a) Develop training curriculum for building
FP advocacy capacities at regional and
district levels
Year 2 Advocacy capacity building
strategy in place
212,204,283

United Republic of Tanzania | National Family Planning Costed Implentantation Program
26
STRATEGIC ACTIVITIES TIMEFRAME SUCCESS INDICATOR
COST
(FY 2010–2016)
2b) Orient representatives from regional and
district councils on FP advocacy
Years 2–4 Advocacy activities led
by district council RH
workers and local FP
stakeholders
84,818,000
Capacity Building Total (in Tshs): 5,683,678,283
1
Addressed in HRHSP 2008–2013, strategic objective 4: To improve Workforce Management and Utilization.
2
Addressed in PHSDP 2007–2017 under the objective Human Resources for Health.
3
Activity included in the central budget for the rst two years to allow districts to incorporate CCHPs in future years.
Resources for this activity in the future will be mobilized through CCHPs.
AGOTA = Association of Gynaecologists and Obstetricians of Tanzania; CCHPs = Council Comprehensive Health
Plans; CTU = contraceptive technology update; MAT = Medical Association of Tanzania; PAT = Paediatric Association
of Tanzania; TAMA = Tanzania Midwives Association.
This SAA refers to strengthened service delivery systems and increased options for delivery of
quality, affordable, and sustainable FP.
Service delivery systems are the organizational components that affect access to family planning
services. They include facility- or clinic-based services, CBS, and other modalities and channels
within and outside of the health sector. Service delivery systems include physical infrastructure,
equipment, and supplies, as well as special considerations and opportunities, such as integration of
services, to meet the needs of vulnerable populations such as youth, men, women receiving PNC or
PAC, or HIV-infected women.
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
Strategic Action 1. Strengthen systems, facilities, infrastructure to support FP services at
appropriate levels
1(a) Ensure availability of equipment,
infrastructure, and supplies for FP
provision (coordination meetings of
RCHS with PHSDP, RHMT, CHMT, and
implementation partners to improve FP
services)
Years 1–6 # of facilities
improved
0
1
1(b) Training on use and maintenance of
equipment and physical structure and
systems
Year 1 Training completed 0
1
1(c) Incorporate plans for health facility
improvement in annual operating plans
Years 1–6 Funds allocated for
facility improvement
0
1
Strategic Action 2. Foster cost-effective integration and referral of FP with HIV, ANC, PNC,
and PAC services for men, women, and youth
2(a) Develop, implement operational tools for
cost-effective integration and referral of FP
with HIV, ANC, PNC, PAC services for men,
women, youth
Year 1 Supporting documents
aligned and ready for
use
96,770,000
2(b) Orient RHMTs and CHMTs on operational
tools in zonal dissemination meetings
Years 2, 5 Meetings held,
materials distributed
55,770,000
2(c) Produce 20,000 copies of logo for branding of
SDPs providing services
Years 1, 3 # logos produced 20,000,000

United Republic of Tanzania | National Family Planning Costed Implentantation Program
27
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
2(d) Brand all public and private SDPs providing
FP services with Green Star Logo
Years 1, 3 # branded SDPs 5,000,000
Strategic Action 3. Strengthen and increase availability of integrated CBS
3(a) Print additional copies of existing CBD
guidelines, training curricula, and job aids
Year 1 # copies produced 17,500,000
3(b) Update guidelines, training curriculum, job
aids, etc. for CBD
Years 3–4 Updated support
materials for CBDs
150,540,000
3(d) Conduct TOTs on guidelines, training
curriculum, job aids, etc for CBD
Years 2, 4 # trained CBD
trainers in each zone
325,215,000
3(e) Training of CBD supervisors Years 2–3 # trained CBD
supervisors per district
328,324,000
3(f) Explore opportunities to increase access
to quality provision of injectables in the
community
Year 3 # completed studies
with findings
implemented
270,000,000
3(g) Supportive supervision from the central level
(integrated)
Years 1–6 # supervision visits 384,000,000
3(h) Expand methods available through
pharmacies, ADDOs, drug shops, social
marketing
Years 2–5 # of new access points
and sales volumes
32,200,000
3(i) Sensitize RMTs and CMTs on introducing or
revitalizing the CBD program
Years 2–3 # of sensitization
meetings held
110,190,000
3(j) Conduct training of 1,500 CBD workers per
year, including youth workers
Years 1–6 # of CBDs trained 0
2
Strategic Action 4. Increase awareness and acceptability of FP services by males
4(a) Conduct situational analysis of male
involvement and participation in FP/SRH
Years 1 Situational analysis
conducted
60,000,000
4(b) Develop print messages and radio spots to be
deployed in all regions
Years 1 # posters radio and
TV spots developed
23,567,500
Strategic Action 5. Increase availability of FP-related YFS
5(a) Update FP trainers on the key strategies on
adolescent YFS and peer education
Year 1 # FP trainers trained
on the provision of
YFS
143,190,000
5(b) Train providers in provision of YFS Year 2 # providers trained
and providing YFS
0
2
Strategic Action 6. Strengthen, expand FP through private sector (includes NGOs, FBOs,
social marketing, commercial sector, private clinics, etc.)
6(a) Assess capacity, qualifications of a sample
of private-sector facilities (FBO, NGO,
commercial) to provide FP services according
to national standards and guidelines.
Year 1 Assessment conducted 60,000,000
6(b) Build capacity and promote provision of
FP services by the private sector, including
increasing the number of facilities registered
for RCH services
Year 1 Inventory of private
sector SDP available;
coordination
mechanism in place
52,432,500
6(c) Orient CHMTs, zonal training institutions,
and APHFTA on the plan and their expected
roles to support its implementation
Years 2, 3 # People oriented on
role of private sector
in FP service provision
95,150,000
6(d) Promote enhanced private sector provision of
FP services
Years 2–5 # People oriented on
role of private sector
in FP service provision
48,607,500

United Republic of Tanzania | National Family Planning Costed Implentantation Program
28
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
6(f) Explore the feasibility for expanding social
marketing of FP products by CBD (formative
research study)
Year 1 Study completed; way
forward documented
60,000,000
Strategic Action 7. Develop, promote, implement approaches to ensure increased access to FP
for low-income and vulnerable groups
7(a) Conduct segmentation analysis to determine
health-seeking attitudes, behaviours, access to
FP by economic quintile
Year 1 Report on health-
seeking attitudes and
behaviours by wealth
quintile
2,400,000
7(b) Research access barriers and establish
means and approaches to enhance service
accessibility among the economically
disadvantaged
Year 2 Report on access
barriers and
recommendations to
overcome them
3,360,000
7(c) Develop advocacy strategy to help overcome
barriers faced by the economically
disadvantaged
Year 3 Changing proportions
in service access by
wealth quintile
1,200,000
Strategic Action 8. Update/revise and disseminate the FP Provision Policy Guidelines and
Standards
8(a) Revise FP Provision Policy Guidelines and
Standards, update supervisory checklist
against updated FP standards and guidelines
Year 1 Updated policy
guidelines and
standards, and
supervisory checklist
34,500,283
8(b) Print and distribute 8,000 copies of the policy
guidelines
Year 2 # policy guidelines
distributed
46,000,000
8(c) Orient DRCHCo, RCHCo, other stakeholders
on the updated FP Policy Guidelines and
supervisory checklists
Year 2 # of DRCHCos and
RCHCos oriented by
zone
48,805,000
Service Delivery Total (in Tshs): 2,213,991,783
1
To be conducted in liaison with the PHSDP 2007–2017.
2
Resources to be mobilized through CCHP.
ADDOs = accredited drug dispensing outlets; ANC = antenatal care; APHFTA = Association of Private Health Facilities
in Tanzania; CBD = community-based distribution; CCHP = Council Comprehensive Health Plan; CHMT = Council
Health Management Team; CMT = Country Management Team; DRCHCo = reproductive and child health coordinator;
PAC = postabortion care; PNC = postnatal care; RCH = reproductive and child health; RCHCo = reproductive and child
health coordinator; RHMT = Reproductive Health Management Team; RMT = Regional Management Team; SDP =
service delivery point; SRH = sexual and reproductive health; TOT = train the trainer; YFS = youth-friendly services.
Reinvigorated advocacy increases the visibility of and support for FP as a key investment for
improving the lives, health, and well-being of Tanzania’s people. This objective addresses the
underlying causes of loss of visibility and momentum in the Tanzania FP program as well as the
knowledge-use gap among FP clients.
Strategic actions proposed are aimed at sustaining support for FP from the highest policy levels and
at promoting public dialogue at all levels, national through community, about the important role of
FP in promoting health and gender equity and supporting development. It also involves addressing
policies that may impede achievement of the other objectives, such as restrictions on what level
of provider is authorized to provide certain contraceptive methods, or how funds for programs are
allocated and channelled.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
29
Addressing the knowledge-use gap will involve addressing myths and misinformation about FP and
fear of side effects and health concerns that impede its adoption and use. Additionally, it addresses
demands for FP that must go beyond maintaining current levels of use and meeting unmet needs if
the One Plan target is to be met.
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
Strategic Action 1. Organize advocacy to prioritize FP with separate budget line for FP
1(a) Review mechanisms of FP budget-
development and resource-allocation
systems
Year 1 Report describing budget-
development & resource-
allocation systems
3,240,000
1(b) Advocacy meetings involving key
stakeholders, PMO-RALG, and MoFEA
officials leading to establishment of a
separate FP budget line item at national,
regional, and district levels
Years 1, 2 Budget line established
at national, regional, and
district levels
10,523,330
Strategic Action 2. Ensure inclusion of FP in major national policy documents, implementation
plans that determine budget allocations, stressing significance of FP to national development
2(a) Conduct a consultation meetings to
ensure inclusion of FP in major national
policy documents, strategies and plans
Years 1, 3 Report from consultation
meeting
6,482,000
Strategic Action 3. Conduct and sustain advocacy targeting development partners and donors
to raise level of FP support
3(a) Mapping of development partners
interested in supporting FP
Year 1 Report on local
development partners’
funding criteria, priorities
20,000,000
3(b) Develop, implement FP resource
allocation advocacy strategy targeting
development partners
Year 2 Resource allocation from
development partners for
FP increases
133,690,330
3(c) Organize two 1-day meetings per year
involving FP stakeholders on repositioning
FP
Years 2–5: Meetings held and
minutes on file indicating
action items
29,986,500
Strategic Action 4. Reposition, reinstate Green Star logo as a National FP program
4(a) Conduct one national relaunch of
the Green Star logo by high-level
governmental official (include launch
materials, e.g., caps, T-shirts, stickers)
Years 1, 2 % of respondents
recognizing the logo as a
symbol of FP (survey)
161,750,000
Strategic Action 5. Conduct sustained national FP advocacy campaign to provide accurate
information, address rumours/misconceptions, promote male involvement, influence social
values, and reach vulnerable groups
5(a) Prepare, produce, broadcast radio spots
(52/yr), radio soap opera “Zinduka
program“ 52 episodes/yr) and TV
programs (52 episodes/spots/yr) on FP
Years 1–6 # radio and TV spots
produced and aired and
estimated listenership
468,000,000
5(b) Produce, distribute revised print materials
(posters, IEC, BCC materials) to all
clinics and training centres
Years 1–6 Qty of materials produced
& distributed by type
1,000,000,000
5(c) Conduct FP campaigns in all ongoing
health campaigns and national festivals
Years 1–6 # overall health campaigns
adapted to include FP
messages
201,300,000
5(d) Revive/orient FP media group to support
a multimedia dissemination campaign
Years 1–6 # articles published per
year
25,396,750

United Republic of Tanzania | National Family Planning Costed Implentantation Program
30
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
Strategic Action 6. Establish a network of community-level champions (community leaders,
religious leaders, politicians) to reassure the population of the acceptability and benefits of FP
6(a) Orient DRCHCo and RCHCo about the
Champions initiative
Year 1 # oriented on Champions
Initiative
123,355,500
6(b) Train zonal trainers on champions
approach
Year 1 # Trainers trained to
support Champions
Initiative
323,980,000
6(c) Support, follow-up districts/regions on
the process to identify, select and recruit
champions (communication costs only)
Year 1 # Champions recruited 200,000
6(d) Orient recruited champions Years 1–3 # Champions trained 1,334,850,000
Strategic Action 7. Establish a network of national-level champions to reassure the population
of the acceptability and benefits of FP
7(a) Identify, select, recruit champions
via consultations between RCHS and
National FP Working Group and other
stakeholders
Year 1 # of Champions in place
and active
100,000
Advocacy Total (in Tshs): 3,638,932,250
BCC = behaviour change communication; DRCHCo = reproductive and child health coordinator; IEC = information,
education and communication; MoFEA = Ministry of Finance and Economic Affairs; PMO-RALG = Prime Minister’s
Ofce–Regional Administration and Local Government; RCHCo = reproductive and child health coordinator; RCHS =
Reproductive and Child Health Section.
Strengthened health systems management and M&E of the national FP program. This objective
addresses the need to reinforce the management capacity at all levels—central, regional, and district
council levels. Effective management systems include ensuring that financial resources are made
available in a timely manner to all implementing levels, coordinating with other governmental
ministries and implementing partners, regular tracking of activities and deliverables needed to
achieve plan objectives, integrating with and using the HMIS, and tracking M&E data to improve
program performance.
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
Strategic Action 1. Strengthen leadership and management capacity at RCHS at all levels
1(a) Organize and conduct a 1-day initial
alignment meeting for 60 key persons from
national, zonal, regional, and district levels
to generate necessary support for the LDP
Year 1 # MoHSW staff who
participate, written
commitment to support
LDP
15,234,750
1(b) Organize and deliver the LDP in three
5-day workshops for six teams of five from
central, zonal, and regional level RCH staff
Years 1, 2 # teams formed with
action plans
148,663,000
1(c) LDP-trained teams prepare for, present
results achieved by implementing
action plans in a 2-day meeting for key
stakeholders
Year 2 end # action plans
implemented yielding
measurable results
26,356,000
1(d) Conduct internal, external study tours to
FP providers to learn best practices
Years 1–6 Documented best
practices, updated
guidelines to support QI
62,304,000

United Republic of Tanzania | National Family Planning Costed Implentantation Program
31
STRATEGIC ACTIVITIES TIMEFRAME
SUCCESS
INDICATOR
COST
(FY 2010–2016)
1(e) Support RCHS staff to attend FP courses
and national/international meetings
Years 1–6 # of RCHS staff who
attended training
courses
154,573,800
1(f) Procure a vehicle for RCHS Year 1 Vehicle procured 270,000,000
Strategic Action 2. Develop, maintain, coordinate, implement an M&E system aligning inputs
to outputs at all levels, national through district
2(a) Conduct rapid assessment of FP services/
data, report to key regional and district staff
to guide design of new reporting framework
(research assessment, 2-day workshop to
share results)
Year 1 Identified gaps in
reporting mechanisms
and data collection
obstacles
30,168,000
2(b) Establish framework, guide, methods for
collecting and reporting RCH/FP data at
district and regional levels
Year 1 Documented framework
for collection and
reporting of data on
RCH/FP indicators
11,386,250
2(c) Provide training at regional and district
levels in strategic planning, using data
to set realistic goals, plan and monitor
program activities
Years 2–3 Key RCH/FP staff
trained in use of data for
planning, monitoring
performance, developing
Annual Action Plans
43,090,000
2(d) Develop, implement executive dashboard
to monitor FP program, NFPCIP
implementation
Years 2, 3 Using executive
dashboard for NFPCIP,
FP programs
86,724,250
Strategic Action 3. Strengthen forums on FP to facilitate exchange of information, leverage
resources, synchronize activities, and share lessons
3(a) Conduct monthly National FP Working
Group meetings
Years 1–6 # National FP working
group meetings held,
documented per year
15,120,000
3(b) Revive and maintain RCHS Web site Years 1–6 Up-to-date FP issues
Web site
168,000,000
3(c) RCHS participates in annual coordination
meetings with zonal level
Years 2–6 RCHS presence
at annual zonal
coordination meetings
54,495,000
Strategic Action 4. Establish existing funding levels and applications (public and private
sectors) as a basis for resource mobilization
4(a) Mapping of current FP system - who
(public, CSOs, NGOs, FBOs) is doing
what, where, when, etc., including
National FP Subaccounts; establish and
maintain database for FP financing (current
and commitments)
Year 1 Report on current
structure of FP services,
source and use of funds
80,000,000
4(b) Disseminate results of National Family
Planning Subaccounts and identify gaps
and opportunities for increasing FP
financing
Year 1 Reports disseminated 13,935,000
4(c) Disseminate information in ongoing
forums at national, regional, and district
levels to enable coordination of activities
and share lessons learned; engage policy
makers, donors
Years 2–6 Functioning cross-sector
forum for sharing hosted
by RCHS
25,825,000
Health Systems Management Total (in Tshs): 1,121,230,800
CSOs = civil society organizations; FBOs: faith-based organizations; LDP = Leadership Development Plan; NGOs =
nongovernmental organizations; QI = quality improvement; RCHS = Reproductive and Child Health Section.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
32
The NFPCIP will be implemented under the leadership and management of existing governance
structures at all levels of the health system. However, the cooperation, input, and actions from a wide
range of partners and stakeholders at all levels are required for success in achieving goals effectively
and efficiently. The NFPCIP will be implemented in collaboration with relevant stakeholders,
which include related ministries and agencies, development partners, the civil society, community-
based organizations (CBOs), professional associations, FBOs, voluntary agencies, and the private
sector, among others. The National Family Planning Working Group is expected to continue to
play an important role during implementation of the NFPCIP over the next six years. The roles and
responsibilities of the many different stakeholders are summarized below.
At the central level, the MoHSW is responsible for overall coordination and oversight of all
aspects of the NFPCIP. This includes responsibility for developing or updating policies that affect
implementation, for resource mobilization, and for monitoring and evaluation. The NFPCIP will be
considered a ‘living document’: as the monitoring and evaluation of implemented activities provide
new information, as changes emerge as a result of the DHS 2009–2010, or as situations evolve, the
MoHSW will be responsible for adjusting the Program to incorporate needed changes. Coordination
also includes ensuring that the strategic actions and activities of the NFPCIP are integrated and
harmonized with and supported by other health-sector programs. Resource mobilization includes
the development of annual budgets in collaboration with the MoFEA and in the context of the
MTEF. It also involves collaboration with development partners, including those who participate in
the sector-wide approach.
Key agencies under the MoHSW also will play crucial roles in implementing the NFPCIP, including
MSD and the Tanzania Food and Drug Authority (TFDA). Close coordination and improvements
in procurement of contraceptive commodities through the MSD are essential to provide adequate
supplies of FP methods for all service delivery partners, in both the public and private sectors.
During the next six years, new, improved, or more cost-effective contraceptive technologies may
become available, and incorporating such new methods into the program will require review and
approval of the TFDA.
A large segment of the NFPCIP is aimed at improving the FP knowledge and skills of health
providers. This includes updating and strengthening the FP components of training through public-
and private-sector training institutions and the Zonal Training Centres.
Health services, including FP, are the responsibility of the MoHSW and of LGAs. Planning
and budgeting for health services delivery has been decentralized to the district level, including
prioritizing the inclusion of FP in CCHPs. As the LGAs assume greater responsibility for planning,
budgeting, and monitoring delivery of services in the communities in their districts, they will
similarly play critical roles in achieving the NFPCIP objectives.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
33
The PMO-RALG directly supervises the LGAs and, with the MoHSW, reviews and assesses the CCHPs.
Reviews pay close attention to ensure the inclusion of FP resources and adequate justification in the
CCHPs before they are approved for funding.
The PMO itself provides overall government coordination, including the coordination of the
government’s response to HIV/AIDS. The Tanzania Commission on AIDS (TACAIDS) operates
under the auspices of the PMO, and it will be instrumental in ensuring the integration of FP as a
key strategy for HIV/AIDS prevention.
The MoFEA collaborates closely with the MoHSW in budget planning, disbursement of funds, and
accounting for expenditures. Improved coordination and communication between the MoFEA and
MoHSW will ensure timely disbursement of funds needed for implementation of the NFPCIP.
The Ministry of Education is responsible for health cadres with university-level training. As
such, this Ministry will be a crucial partner in ensuring the inclusion of evidence-based FP curricula
in pre-service training for health personnel in collaboration with the MoHSW.
Included in this category are the bilateral and multilateral donors. Also included in this category
is a host of implementing partners that provide technical assistance and expertise in support of the
national FP program. Donor agencies will be called upon to increase their support and to augment
the resources that will be required for the NFPCIP.
Implementing Partner will continue to be called upon by and under the coordination of the
MoHSW for their wide variety of expertise. These reflect all five of the SAAs and will be drawn
from experiences in Tanzania and throughout the world to ensure that the implementation of the
NFPCIP reflects state-of-the-art information and interventions.
Although about 80 percent of FP services are provided through the public sector, a number of
NGOs and FBOs also play important roles in service delivery. As such, they are critical partners
in implementing the NFPCIP. The FBOs are important sources of broader health care, especially
in some rural areas of Tanzania, and many of them include FP as components of their services. The
MoHSW will continue to look to these partners in implementing the NFPCIP. This includes ensuring
coordination and training, procurement of contraceptive commodities, and ensuring adherence
to set service standards and guidelines. These organizations are also expected to contribute their
service data for M&E, to assist the MoHSW in maintaining a comprehensive picture of NFPCIP
implementation, as well as identifying needs and opportunities to expand services.
The level of resources that will be required for successful implementation of the SAAs to reposition
FP and achieve the One Plan target for FP will need to expand considerably and quickly. The
main sources of funding for the current program include the Tanzanian government; the Basket
funds managed through the MTEF, through which most multilateral and bilateral donors currently
contribute; and ‘out-of-basket’ funds from a few donors, most notably the United States Agency for
International Development (USAID). Other sources of support include funding from NGOs and
FBOs as well as costs recovered through fees for service by private-sector providers.

United Republic of Tanzania | National Family Planning Costed Implentantation Program
34
In implementing the NFPCIP, the MoHSW will provide guidance to ensure that annual budget
requests to the MTEF from the district levels include FP, so that Basket funds can be used to support
FP. Improving understanding of the budgeting process, as well as increasing the level of priority for
FP at the district level are both key recommended implementation actions of the NFPCIP that can
help to address this resource mobilization challenge. Recent recommendations from the Tanzania
Parliamentary Association for Population and Development call for a larger portion of Basket funds
to be spent on FP commodities, and for creating an independent FP budget line item in the budget
guidelines. Such actions are currently underway under the leadership of the MoHSW.
Expanding involvement of the private sector, including building on current social-marketing
programs, will also be promoted to increase resources for FP. NGOs and FBOs can also play a greater
role by mobilizing and allocating resources for implementing the NFPCIP.
Managing and implementing the NFPCIP effectively will require a carefully developed and
implemented framework and system for M&E. Although the M&E framework and indicators should
link with the national HMIS, the HMIS includes only a limited number of indicators for FP. Hence,
tools to collect monitoring data must be updated to include a comprehensive list of FP indicators.
Because of the many activities and inputs that must be tracked to ensure timely and effective
implementation of the NFPCIP, a management monitoring tool to track implementation of the
strategic activities and achieving the objectives of the NFPCIP will be developed.
The M&E framework can be used routinely at several levels, including the government, the FP
Working Group, development partners, and donors to track achievement of the implementation
actions and activities, to identify problem areas in implementation or shortfalls in resources.
Developing and applying an M&E framework has been facilitated by the inclusion in the NFPCIP
of success indicators for each implementation action and the activities and steps expected to be
carried out under each. Success indicators for the NFPCIP are expressed in terms of outputs and
outcomes to be achieved by each activity. Ultimately, successful implementation of the NFPCIP
must be measured in terms of its effect on contraceptive prevalence, but measuring the effect is
beyond the capacity of the proposed M&E system and is instead provided by the DHS, which will
occur next in 2009–2010 and 2014–2015.
Finally, the implementation actions and activities recommended in the NFPCIP are evidence-
based. Over the five years of implementing the NFPCIP, however, new issues and questions will
undoubtedly arise about the most cost-effective alternatives for implementation, or additional
evidence will be required as a basis for scale-up of program components. These issues and questions
can help to inform a research agenda to support continued innovation and ensure a sound, evidence-
based program to reach the NFPCIP targets.
