
I
ran has experienced dramatic demographic
change in the last decade. Levels of childbear-
ing have declined faster than in any other
country, and maternal and child health have great-
ly improved. These changes have coincided with
the revival of the national family planning pro-
gram, which is delivered through a nationwide
network of primary health care facilities. Many
observers have wondered how such a dramatic
increase in contraceptive use could have occurred
in a traditional society ruled by Islamic law.
Demographic Trends
Iran’s population increased from 34 million in
1976 to nearly 50 million in 1986, with an aver-
age growth rate of 3.9 percent per year (3.2 per-
cent from natural increase and 0.7 percent from
immigration); a decade earlier, the average annual
growth rate had been 2.7 percent. But the rise in
the population growth rate that occurred during
and after the 1979 Islamic revolution in Iran was
followed by a sharp decline. Between 1986 and
1996, the population growth rate dropped to 2.0
percent per year.
1
Currently, Iran’s population is
estimated to be growing by 1.2 percent a year.
The population growth rate has been declin-
ing because of the dramatic change in Iranian
women’s fertility: According to the Iranian min-
istry of health, the country’s total fertility rate
declined from 5.6 births per woman in 1985 to
2.0 births in 2000 (Figure 1). Iran’s fertility
decline is particularly remarkable in how quickly
it occurred in rural areas. Between 1976 and
2000, the total fertility rate in rural areas declined
from 8.1 births per woman to 2.4 births per
woman. The fertility of urban women declined
from 4.5 births to 1.8 births per woman during
the same period.
2
Figure 2 (page 2) shows how
fertility rates in Iran vary by province.
The decline in fertility has mainly been due
to the increase in contraceptive use among mar-
ried women: In 2000, 74 percent of married
women practiced family planning, up from 37
percent in 1976. The change in marriage patterns
has also affected fertility: Women’s average age at
first marriage increased from 19.7 in 1976 to
22.4 in 1996.
IRAN’S FAMILY PLANNING PROGRAM:
RESPONDING TO A NATION’S NEEDS
POPULATION REFERENCE BUREAU
by Farzaneh Roudi-Fahimi
Iran MoroccoEgypt Turkey
1985 2000 1987 19971988 2000 1988 1998
5.6
2.0
4.4
3.5
4.8
3.2
3.0
2.6
Births per woman
Figure 1
Trends in Total Fertility Rates for
Selected Countries
NOTE: Rates for Iran are based on data from the ministry of health and
medical education. The Statistical Center of Iran has reported that fertility
fell from 7.1 births per woman in 1986 to 2.5 births per woman in 2001.
SOURCE: Population Reference Bureau database, based on selected
national surveys.
This overview of Iran’s family planning efforts and the role of the Islamic government and civil
society in the revival of the national family planning program is the second in a series of policy briefs
from the Population Reference Bureau. This series analyzes population, environment, reproductive
health, and development linkages within the framework of the Cairo Programme of Action and the
cultural contexts of population groups in the Middle East and North Africa (MENA). Future briefs
on MENA will cover specific population-related topics or country case studies.

Evolution of Iran’s Family
Planning Program
There are three distinct periods in the history of
Iran’s family planning program, each marked by
major changes in the government’s policy.
3
Family Planning Before the 1979 Islamic
Revolution
Iran was one of the first countries to establish a
family planning program as part of its develop-
ment plan. The Imperial Government of Iran
adopted a national family planning policy in
1966, and launched an active family planning
program in the ministry of health in 1967. The
1967 Tehran Declaration acknowledged family
planning as a human right and emphasized its
social and economic benefits for families and soci-
ety.
4
The program recruited and trained a cadre of
professional staff, and taught many young doctors
about family planning’s implications for public
health and its critical role in improving the well-
being of women and children.
Family planning became an integral part of
maternal and child health services nationwide. By
the mid-1970s, 37 percent of married women
were practicing family planning, with 24 percent
using modern methods. The total fertility rate,
although declining, remained high, at more than
six births per woman.
The Islamic Revolution and Pronatalism
The family planning program was dismantled soon
after the 1979 Iranian Revolution, because the
program was associated with the Iranian royal
family and was viewed as a Western innovation.
The new government advocated population
growth, and adopted new social policies, including
benefits such as allowances and food subsidies for
larger families. In an attempt to ensure continued
government support for family planning, a num-
ber of committed health professionals approached
the government with information about the health
benefits of family planning. They even obtained
fatwas (religious edicts concerning daily life) from
Imam Khomeini and other top-ranking clerics to
the effect that “contraceptive use was not inconsis-
tent with Islamic tenets as long as it did not jeop-
ardize the health of the couple and was used with
the informed consent of the husband.”
5
In 1980, Iran was attacked by Iraq. During
the eight-year conflict that followed, having a large
population was considered an advantage, and
population growth became a major propaganda
issue. Many Iranian officials were pleased when the
1986 census showed that Iran’s population of close
to 50 million was growing by more than 3 percent
per year, one of the highest rates in the world.
6
At the same time, the Plan and Budget
Organization, which is the main government
agency responsible for monitoring government
revenues and expenditures, and other ministries,
such as health, education, and agriculture, were
aware of the economy’s vulnerability and the
added difficulties caused by a rapidly growing
young population. To assess the economic dam-
ages of the war and prepare for a national devel-
opment plan, the Plan and Budget Organization
collected data on issues such as employment and
demand for basic services. The assessment painted
a grim picture of the country’s economy.
PRB MENA Policy Brief 2002
2
SISTAN-BALUCHISTAN
KERMAN
FARS
KHUZISTAN
ILAM
MARKAZY
QOM
HAMADAN
GHAZVIN
ZANJAN
KURDISTAN
ARDEBIL
GILAN
YAZD
ESFAHAN
GOLESTAN
KHORASAN
B
O
O
S
H
E
H
R
HORMOZGAN
TEHRAN
LORISTAN
SEMNAN
MAZANDARAN
AZARBAIJAN E.
CHAHARMAHAL
KOHGILUYEH
Births per woman
A
Z
A
R
B
A
IJ
A
N
W
.
KERMANSHAH
1.4–2.2 (Below or at replacement)
2.3–2.9
3.0 and up
Figure 2
Total Fertility Rate by Province, Iran, 2000
SOURCE: Iranian Ministry of Health and Medical Education et al., Demographic and Health Survey,
Iran 2000, Preliminary Draft Report (2002).

After the war with Iraq ended in 1988, as the
government began to prepare its first national
development plan, the Plan and Budget Organiza-
tion alerted top government leaders that the
nation’s dwindling resources could not both sup-
port the high cost of reconstruction and provide
the social and welfare services stipulated by the
new constitution. In response, the prime minister
asked all government departments to review the
population growth rate’s impact and implications
for the first development plan (which would
take effect in 1989). Later, he declared that the
government was “reconsidering the issue of
population growth.”
7
Restoring the Family Planning Program
Having convinced many top policymakers of the
importance of family planning, the Plan and
Budget Organization and the ministry of health
and medical education decided to launch a publici-
ty campaign to convince other members of the pol-
icy elite and the general public about the need for a
national population policy. The much-publicized
three-day Seminar on Population and Development
was held in Mashad in September 1988.
The Iranian media helped disseminate the
seminar’s main message: Iran’s population growth
rate was too high and, if left unchecked, would
have serious negative effects on the national econo-
my and the welfare of the people. Participants at
the seminar strongly urged the government to con-
sider population issues during policymaking. At a
press conference at the end of the Mashad seminar,
the minister of health and medical education reit-
erated the late Imam Khomeini’s fatwa regarding
family planning, and announced that the Islamic
Republic of Iran would establish a family planning
program. In December 1988, the High Judicial
Council declared that “there is no Islamic barrier
to family planning.”
8
The Mashad seminar was mainly a profes-
sional and technical gathering; the influential
clergy (ulama) outside the central government
were not involved in the seminar’s deliberations.
To ensure that the proposed policy would have
the clergy’s support, family planning was singled
out for special consideration and discussion at the
February 1989 seminar on “Islamic Perspectives
in Medicine,” which was attended by eminent
clergy and physicians.
Despite these efforts, some influential clergy
were not convinced about the potential effects of
rapid population growth or that public investment
in family planning was consistent with the basic
tenets of Islam.
9
To overcome these objections, the
government took the issue to the Expediency
Discernment Council of the System, which resolves
disputes between parliament and the Guardian
Council. The Expediency Council confirmed that
family planning and population policies were legiti-
mate areas for government involvement, paving the
way for the reintroduction of a national population
policy and the family planning program.
The Revitalized Family
Planning Program
The family planning program, officially inaugu-
rated in December 1989, has three major goals: to
encourage families to delay the first pregnancy
and to space out subsequent births; to discourage
pregnancy for women younger than 18 and older
than 35; and to limit family size to three children.
The ministry of health and medical education has
been given almost unlimited resources to provide
free family planning services to all married cou-
ples, promote small families as the norm, and help
couples prevent unplanned pregnancies. All mod-
ern contraceptive methods are available to married
couples, free of charge, at public clinics. In 1990,
to remove continuing doubts about the accept-
ability of sterilization as a method of family plan-
ning, the High Judicial Council declared that
sterilization of men and women was not against
Islamic principles or existing laws.
In 1993, the legislature passed a family plan-
ning bill that removed most of the economic
incentives for large families. For example, some
allowances to large families were cancelled, and
some social benefits for children were provided for
only a couple’s first three children. The law also
gave special attention to such goals as reducing
infant mortality, promoting women’s education
and employment, and extending social security
and retirement benefits to all parents so that they
would not be motivated to have many children as
a source of old age security and support.
While all these legal reforms in support of the
family planning program are significant, high-
lighting Iran’s commitment to slowing population
growth, there has been no assessment of the laws’
PRB MENA Policy Brief 2002
3

implementation or their impact on lowering fertil-
ity. The level and speed of the decline in fertility
have been beyond any expectation. The first offi-
cial target of the revitalized family planning pro-
gram, as reflected in the government’s first
five-year development plan, was to reduce the
total fertility rate to 4.0 births per woman by
2011.
10
By 2000, the rate was already down to
half the stated goal, at 2.0 births per woman.
Population and health experts close to the
program attribute its success largely to the govern-
ment’s information and education program and to
a health care delivery system that was able to meet
reproductive health needs. Family planning is one
of many health services provided by the system,
which is based on different levels of care and an
established referral system (see Box 1 for more on
care delivery in rural areas). Overall family plan-
PRB MENA Policy Brief 2002
4
Iran’s rural health care network is the cornerstone of the
country’s health care system. The network evolved out
of a series of pilot projects that were conducted in the
early 1970s as part of an effort to find the best system
for expanding medical and health services in rural areas.
(Iran’s rural population is widely dispersed: In 1996,
more than 68,000 villages had an average population
of 340 people.) The result was the establishment of
rural “health houses,” based on the idea that vaccine-
preventable diseases, acute respiratory infections, and
diarrheal diseases can be addressed by making simple
technology and information available to even minimally
trained personnel.
There are now more than 16,000 health houses in
Iran, covering around 95 percent of the rural population;
mobile clinics bring health services to people living in
remote areas. Each health house serves around 1,500
people, usually consisting of the people of one central
village (where the health house is located) and those of
satellite villages that are within an hour’s walk from the
central village. Each health house generally has two
health providers (in principle, one man and one
woman), known as behvarzes, who receive two years of
training. The female behvarz is in charge of maternal and
child health care, and the male is responsible for issues
related to environmental health, such as water safety and
agricultural production. Behvarzes must be local resi-
dents; the requirement is particularly important for
women behvarzes, who can continue to live in their
home village while working. Since behvarzes are local,
they tend to stay in the job and to know their clients.
One of the first tasks of a behvarz team is to take a
population census of the villages for which their health
house is responsible. The census is repeated at the
beginning of each Iranian calendar year (March 21).
The age and sex profiles of each village are put in charts.
Summary tables of these data are posted on the wall of
each health house and are updated each month. For
example, data can show the number of children who
have been born since the beginning of the year, the pro-
portion who have been vaccinated, and the number who
died, by cause of death. The data also show the number
of married women of reproductive age and their contra-
ceptive prevalence rate by method. Behvarzes are proac-
tive: They are comfortable knocking on people’s doors
to talk about families’ health care needs, including fami-
ly planning, and to give them appointments to visit the
health house.
Box 1
Iran’s Rural Health Care Network
Rural health providers, know as behvarzes, maintain up-
to-date records on the health and well-being of people in
rural villages. Here, two behvarzes from central Iran are
shown in front of their clinic’s charts on local health.
FARZANEH ROUDI-FAHIMI
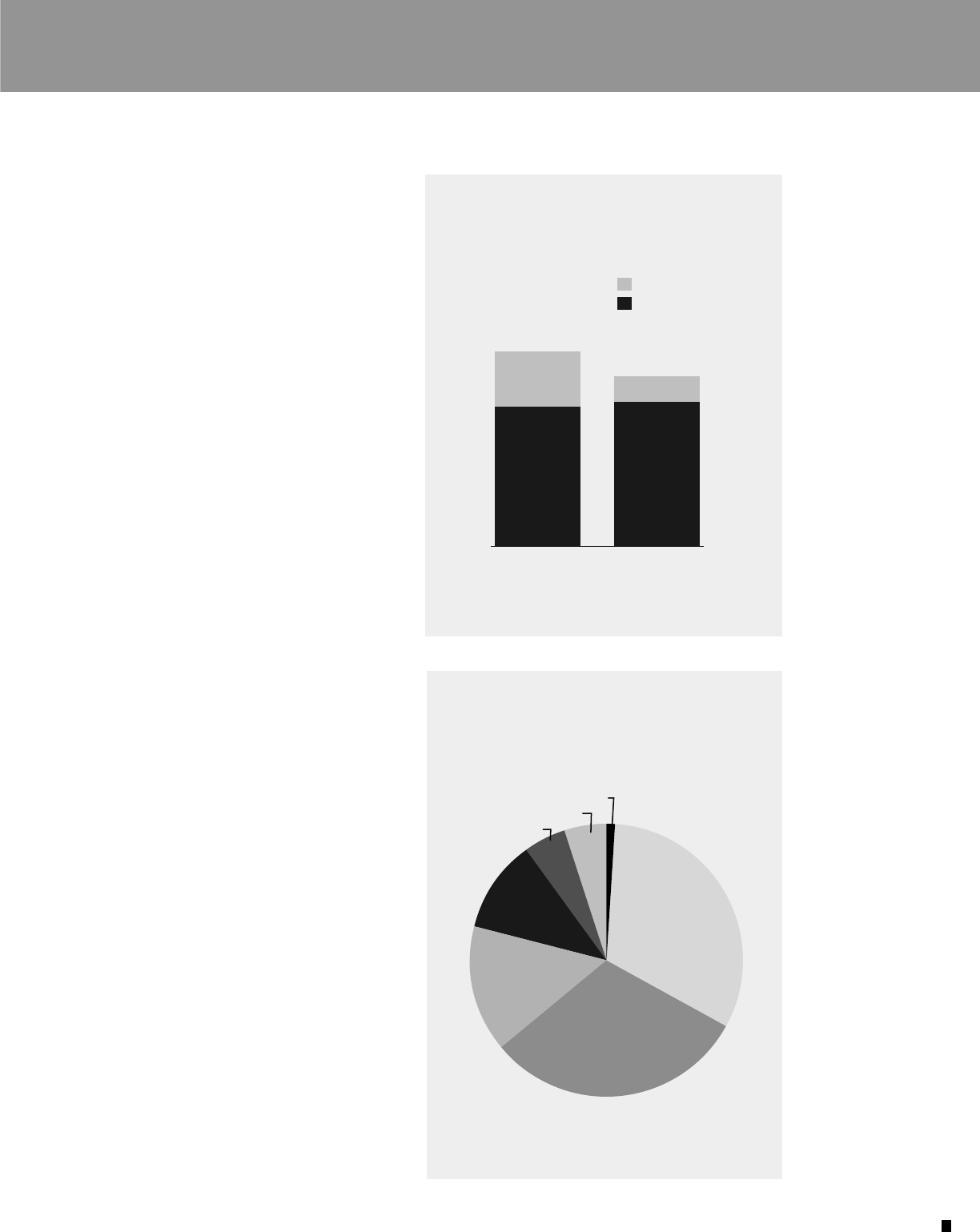
ning practice is higher among women living in
urban areas than among those living in rural areas,
but the use of modern contraceptive methods is
about the same in both urban and rural areas
(see Figure 3). Contraceptive pills are the most
popular modern method, followed by female
sterilization (see Figure 4).
The program has succeeded in removing both
cultural and economic barriers to family planning,
and the information and education campaign has
assured the public that family planning is consis-
tent with Islamic tenets and does not threaten
family values (see Box 2, page 6). By providing
free family planning services, the program has
given low-income couples in both rural and urban
areas access to services that would otherwise be
too expensive for most families. In 2000, the min-
istry of health and medical education provided 75
percent of all family planning services (91 percent
of services in rural areas and 67 percent of services
in urban areas). The question the ministry now
faces is whether the government needs or can even
afford to continue to be so involved in providing
family planning services, since small families and
contraceptive use are now the norm. In the next
10 years, the number of reproductive-age women
will grow by more than 20 percent.
Population education is part of the curricu-
lum at all educational levels; university students,
for example, must take a two-credit course on
population and family planning. Family planning
is also included in the country’s adult literacy
campaign. Couples who are planning to marry
must participate in government-sponsored family
planning classes before receiving their marriage
license. The classes are mandatory for both
prospective brides and grooms, supporting the
family planning program’s goal of increasing male
involvement and responsibility in family planning.
The family planning program, which is attempt-
ing to increase men’s participation in family plan-
ning, uses more than just education to support
men’s involvement: The Middle East’s only con-
dom factory operates in Iran.
One challenge facing the family planning pro-
gram is addressing the regional differences in con-
traceptive use. Generally, the lowest levels of
contraceptive use are seen in the least developed
provinces. Women living in Sistan–Baluchestan
PRB MENA Policy Brief 2002
5
Norplant 1%
Pills
33%
Female sterilization
31%
IUDs
15%
Condoms
10%
Injections 5%
Male sterilization 5%
Figure 4
Contraceptive Methods Used by Married
Iranian Women Who Rely on Modern
Methods, 2000
SOURCE: Iranian Ministry of Health and Medical Education et al.,
Demographic and Health Survey, Iran 2000, Preliminary Draft
(Tehran: Iranian Ministry of Health and Medical Education, 2002).
22%
10%
57%
55%
77%
67%
Urban Rural
Traditional
Modern
Figure 3
Percent of Married Iranian Women
Who Reported Using Different Types of
Contraception, by Region, 2000
SOURCE: Iranian Ministry of Health and Medical Education et al.,
Demographic and Health Survey, Iran 2000, Preliminary Draft
(Tehran: Iranian Ministry of Health and Medical Education, 2002).

province have the lowest rate of contraceptive use
(42 percent), followed by women living in
Hormozgan (55 percent). These two provinces are
among the least developed in the country. The
highest rates of contraceptive use are seen in more
developed regions: In Tehran City, 82 percent of
married women use contraceptives (see Box 3,
page 7, for more on health care in cities).
Another challenge facing the family planning
program is dealing with unplanned pregnancies.
According to the 2000 Demographic and Health
Survey (DHS), 5.2 percent of married women
ages 15 to 49 were pregnant. Of those women,
one-quarter reported that their pregnancies were
unplanned, often due to contraceptive failure. The
highest failure rates occurred with the traditional
methods (withdrawal is the main traditional
method practiced in Iran) and oral contraceptives.
The family planning program is expanding its
services to provide couples with emergency con-
traception. Abortion is illegal in Iran, except to
save the mother’s life, but postabortion care is
provided as part of primary health care.
Family Planning and Other
Development Trends
Although Iran’s Islamic government justified revi-
talizing the family planning program mainly on
macroeconomic grounds, Iranian families needed
little convincing. Iranian society is becoming
PRB MENA Policy Brief 2002
6
“Fewer children, better
education.”
“Less population, more opportunities,
prosperous future.”
“Better life with fewer children:
Girl or boy, two is enough.”
Box 2
Posters From Iran’s Family Planning Program
Iran’s family planning program uses a variety of messages to encourage couples to have smaller
families, emphasizing benefits for both individual families and society as a whole.

increasingly modern and even somewhat Western-
ized; both consumerism and media exposure are
rising. According to the 2000 DHS, 77 percent of
rural households and 94 percent of urban house-
holds had televisions, which had helped promote
the idea of a small family norm.
Improvements in female education have also
contributed to increased use of contraceptives.
The percentage of rural women who were literate
increased from 17 percent to 62 percent between
1976 and 1996; more than 75 percent of Iranian
women are literate. The rate of secondary school
enrollment has more than doubled for girls, from
36 percent in the mid-1980s to 72 percent in the
mid-1990s, while boys’ enrollments have
increased from 73 percent to 81 percent over the
same time span. In 2000, more women than men
entered universities. The longer women stay in
school, the higher the standard of living they want
for themselves and their families. The quality of
children’s lives also becomes more important.
Maternal and child health in Iran has
improved significantly. Maternal deaths due to
pregnancy and childbirth declined from 140
deaths per 100,000 live births in 1985 to 37
deaths per 100,000 live births in 1996. According
to the 2000 DHS, more than 90 percent of preg-
nant women receive at least two prenatal check-
ups, 95 percent of births are attended by a doctor
or trained midwife, and childhood vaccination is
almost universal. Between 1985 and 1996, the
mortality of children under 5 years of age dropped
from 70 deaths to 33 deaths per 1,000 live births,
and the infant mortality rate declined from 51
deaths to 26 deaths per 1,000 live births.
11
Conclusion
The Iranian experience challenges the current
assumption that demographic transition in the
Middle East and North Africa has generally been
slow. The dramatic drop in Iran’s growth rate also
raises questions as to whether the Iranian experi-
ence is unique in part because of specific charac-
teristics of Iranian society, such as the fact that the
great majority of Iranians are Shiite Muslims, who
represent a minority of Muslims worldwide.
However, the changes in Iran confirm that
committed policy and financial support, easily
available family planning services, and strong
demand can ensure that the uptake in contracep-
tive use and decline in fertility occurs very fast.
The Iranian experience highlights three key
points:
■ If family planning programs are to succeed in
Muslim countries, religion must be addressed
carefully and in a culturally sensitive manner.
PRB MENA Policy Brief 2002
7
Box 3
Women Volunteers in Cities
The health care system in rural areas of Iran is proactive in
reaching clients, but the system in urban areas often is not.
To encourage low-income residents of cities to use health
facilities, the government has developed a women’s volunteer
program. The volunteers serve as intermediaries between
families and government-sponsored health clinics. Volunteers
can also choose to participate in other areas of community
life, such as cleaning up the streets or holding classes on spe-
cial health topics.
The women’s volunteer program began in 1993 with
200 volunteers in Shahre-Rey, a low-income suburb south of
Tehran. Now there are more than 43,000 such volunteers
throughout the country, working closely with their neighbor-
hood clinics. Volunteers maintain files of demographic and
health information on each household in their area. The files
are kept at the clinic and can be used by health staff, and
volunteers use the information to help families make
appointments to address health care needs.
Urban health centers use volunteers, who are chosen in part
based on their reputation within the neighborhood, to ensure
that even low-income families receive basic health services.
FARZANEH ROUDI-FAHIMI

POPULATION REFERENCE BUREAU
1875 Connecticut Ave., NW, Suite 520, Washington, DC 20009 USA
Tel.: (202) 483-1100
■
Fax: (202) 328-3937
■
E-mail: popref
@
prb.org
Website: www.prb.org
■ Investments in health infrastructure and
human development are essential in making
family planning programs sustainable.
■ Those who assess population data can play a
key role in educating policymakers about the
likely impact of policy changes.
References
1
The Statistical Center of Iran, Iran Statistical Yearbook 1379
(March 2000–March 2001): Table 2.1.
2
United Nations Population Fund (UNFPA), Country Report
on Population, Reproductive Health and Family Planning
Program in the Islamic Republic of Iran (Tehran: Family
Health Department, Undersecretary for Public Health,
Ministry of Health and Medical Education, 1988); and
Iranian Ministry of Health and Medical Education et al.,
Demographic and Health Survey, Iran 2000: Preliminary Draft
Report (Tehran: Iranian Ministry of Health and Medical
Education, 2002).
3
Amir H. Mehryar, “Repression and Revival of the Family
Planning Program and Its Impact on Fertility Levels in the
Islamic Republic of Iran,” ERF Working Paper 2022 (Cairo:
Economic Research Forum for the Arab Countries, Iran and
Turkey, 2000).
4
Farzaneh Roudi, “Iran’s Revolutionary Approach to Family
Planning,” Population Today 27, no. 7 (1999).
5
Amir H. Mehryar, “Ideological Basis of Fertility Changes in
Post-Revolutionary Iran: Shiite Teachings vs. Pragmatic
Considerations” (Tehran: Institute for Research on Planning
and Development, 2000): 18.
6
Akbar Aghajanian, “Family Planning Program in Iran,”
accessed online at http://spacer.uncfsu.edu/f_aghajanian/
papers/familyplanning.pdf, on May 7, 2002.
7
H. Moosavi, “Without Population Control We Cannot Do
Any of the Other Programs,” Iran Times, April 28, 1989.
8
Mehryar, “Ideological Basis of Fertility Changes in Post-
Revolutionary Iran”: 27.
9
M.A. Ayazi, “Islam and Family Planning” (Tehran: Daftar
Nashr Farhang Islami, 1994); and Ayalullah Muhammad
Hussein Hosseini Tehrani, “Treatise on Marriage: Population
Decline, a Heavy Blow to the Body of Muslims” (Tehran:
Hekmat Publications, 1994).
10
A Summarized Version of the First Five-Year Economic,
Social, and Cultural Development Plan of the Islamic Republic
of Iran (1989-1993), Ratified by the Islamic Consultative
Assembly on January 31, 1990 (New York: Population Policy
Data Bank, United Nations, 1990).
11
UNFPA, Country Report on Population, Reproductive Health
and Family Planning Program in the Islamic Republic of Iran.
Acknowledgments
Farzaneh (Nazy) Roudi-Fahimi of the Population
Reference Bureau prepared this policy brief with assistance
from PRB staff. Thanks are due to Amir H. Mehryar, of the
Institute for Research on Planning and Development in Iran,
for his contribution to the discussions of the policy environ-
ment; to K. Shadpoor, of the Iranian ministry of health, for
his contribution to the discussions of the status of primary
health care in Iran; and to B. Delavar, director general of the
Iranian ministry of health’s directorate of family health and
population, for his comments. Thanks are due to those who
reviewed the brief: Tom Merrick, of the World Bank; B.
Delavar; M.J. Abbasi-Shavazi, of the University of Tehran;
and Akbar Aghajanian, of Fayetteville State University.
This work has been funded by the Ford Foundation.
Design/Production: Heather Lilley, PRB
Managing Editor: Helena Mickle, PRB
© June 2002, Population Reference Bureau
PRB’s Middle East and North Africa Program
The goal of the Population Reference Bureau’s Middle East and
North Africa (MENA) Program is to respond to regional needs for
timely and objective information and analysis on population, socio-
economic, and reproductive health issues. The program raises aware-
ness of these issues among decisionmakers in the region and in the
international community, in hopes of influencing policies and
improving the lives of people living in the MENA region.
MENA program activities include producing and disseminating
both print and electronic publications on important population,
reproductive health, environment, and development topics (many
publications are translated into Arabic); working with journalists in
the MENA region to enhance their knowledge and coverage of popu-
lation and development issues; and working with researchers in the
MENA region to improve their skills in communicating their
research finding to policymakers and the media.
MENA Policy Briefs:
“Population Trends and Challenges in the Middle East and North
Africa” (October 2001)
“Iran’s Family Planning Program: Responding to a Nation’s Needs”
(June 2002)
“Finding the Balance: Water Scarcity and Population Demand in the
Middle East and North Africa” (July 2002)
These policy briefs are available on PRB’s website (www.prb.org),
and also can be ordered free of charge to audiences in the MENA
region by contacting the Population Reference Bureau via e-mail
(prborders@prb.org) or at the address below.
The Population Reference Bureau is the leader in providing timely and
objective information on U.S. and international population trends and
their implications.
